Dolphin
Senior Member (Voting Rights)
https://link.springer.com/article/10.1007/s11011-024-01428-2
12-week melatonin intake attenuates cardiac autonomic dysfunction and oxidative stress in multiple sclerosis patients: a randomized controlled trial
Abstract
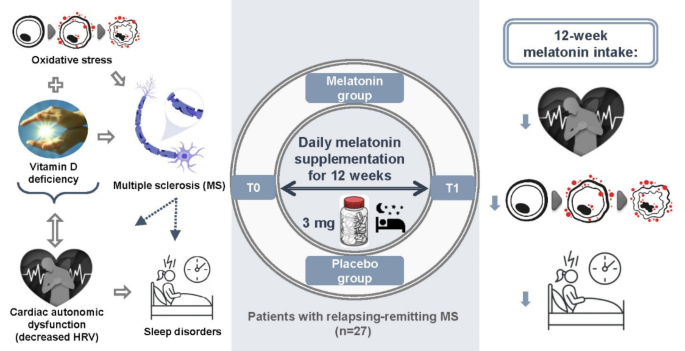
Multiple sclerosis (MS) can induce cardiac autonomic dysfunction identified by a decreased heart rate variability (HRV) which was linked to oxidative stress, vitamin D deficiency and sleep disturbance.
Previous MS studies revealed the antioxidant and anti-inflammatory effects of exogenous melatonin, as well as its benefits on sleep and vitamin D.
We aimed to investigate the change in HRV, oxidative stress, systemic inflammation and sleep following melatonin supplementation in MS patients.
Participants were randomly allocated to either a melatonin group (MG, n = 15) or a placebo group (PG, n = 12) (3 mg/night during 12 weeks).
Pre- and post-tests included HRV analysis (Kubios software), sleep dairy and biological analysis [oxidative stress biomarkers (malondialdehyde (MDA), advanced oxidation protein products (AOPP) and reduced glutathione (GSH)); 25-hydroxyvitamin D; C-reactive protein and cholinesterase Gen.2 (CHE2)].
Based on the pre-post supplementation change (Δ (T1₋T0)), melatonin increased the root mean square of successive differences between normal heartbeats [ΔMG (14.17 ± 16.93) vs. ΔPG (₋8.61 ± 12.67), p = 0.0007] and the HRV high-frequency band [ΔMG (6.86 ± 14.85) vs. ΔPG (₋12.58 ± 13.30), p = 0.0016] comparatively with placebo. MG showed a decrease in the HRV low-frequency band [ΔMG (₋4.96 ± 10.08) vs. ΔPG (10.22 ± 13.54), p = 0.003] as well as in the MDA [ΔMG (₋2.27 ± 1.92) vs. ΔPG (0.22 ± 2.30), p = 0.005] and AOPP levels [ΔMG (₋113.97 ± 137.72) vs. ΔPG (156.46 ± 230.52), p = 0.0008] compared with PG.
Melatonin enhanced the GSH [ΔMG (10.51 ± 14.93) vs. ΔPG (₋5.05 ± 10.18), p = 0.004] and CHE2 levels [ΔMG (407.07 ± 723.26) vs. ΔPG (₋22.92 ± 506.52), p = 0.029] as well as sleep quality [scores: ΔMG (1.50 ± 1.28) vs. ΔPG (₋1.05 ± 2.05), p = 0.0006] and quantity [weighted total sleep time: ΔMG (0.74 ± 1.14) vs. ΔPG (₋1.04 ± 1.00), p = 0.0003] comparatively with placebo.
Caregivers may recommend 12-week nocturnal melatonin intake to attenuate cardiac autonomic dysfunction, oxidative stress and sleep disorders in MS patients.
Clinical registration This study was prospectively registered in the Pan African Clinical Trial Registry database (PACTR202007465309582) on 23 July 2020 (https://pactr.samrc.ac.za/.).
Graphical abstract
Highlights
• 12-week melatonin supplementation (3 mg per night) alleviated cardiac autonomic dysfunction (i.e., it increased heart rate variability) in multiple sclerosis patients.
• Exogenous melatonin had benefits on oxidative stress biomarkers (reduced glutathione, malondialdehyde and advanced oxidation protein products).
• Chronic nocturnal melatonin intake enhanced sleep quality, efficiency and quantity.
12-week melatonin intake attenuates cardiac autonomic dysfunction and oxidative stress in multiple sclerosis patients: a randomized controlled trial
- Research
- Published: 04 December 2024
- Volume 40, article number 52, (2025)
- Cite this article
Metabolic Brain Disease
- Sonda Jallouli,
- Dana Jallouli,
- Mariem Damak,
- Salma Sakka,
- Sameh Ghroubi,
- Chokri Mhiri,
- Tarak Driss,
- Giovanni de Marco,
- Fatma Ayadi &
- Omar Hammouda
17 Altmetric
Abstract
Multiple sclerosis (MS) can induce cardiac autonomic dysfunction identified by a decreased heart rate variability (HRV) which was linked to oxidative stress, vitamin D deficiency and sleep disturbance.
Previous MS studies revealed the antioxidant and anti-inflammatory effects of exogenous melatonin, as well as its benefits on sleep and vitamin D.
We aimed to investigate the change in HRV, oxidative stress, systemic inflammation and sleep following melatonin supplementation in MS patients.
Participants were randomly allocated to either a melatonin group (MG, n = 15) or a placebo group (PG, n = 12) (3 mg/night during 12 weeks).
Pre- and post-tests included HRV analysis (Kubios software), sleep dairy and biological analysis [oxidative stress biomarkers (malondialdehyde (MDA), advanced oxidation protein products (AOPP) and reduced glutathione (GSH)); 25-hydroxyvitamin D; C-reactive protein and cholinesterase Gen.2 (CHE2)].
Based on the pre-post supplementation change (Δ (T1₋T0)), melatonin increased the root mean square of successive differences between normal heartbeats [ΔMG (14.17 ± 16.93) vs. ΔPG (₋8.61 ± 12.67), p = 0.0007] and the HRV high-frequency band [ΔMG (6.86 ± 14.85) vs. ΔPG (₋12.58 ± 13.30), p = 0.0016] comparatively with placebo. MG showed a decrease in the HRV low-frequency band [ΔMG (₋4.96 ± 10.08) vs. ΔPG (10.22 ± 13.54), p = 0.003] as well as in the MDA [ΔMG (₋2.27 ± 1.92) vs. ΔPG (0.22 ± 2.30), p = 0.005] and AOPP levels [ΔMG (₋113.97 ± 137.72) vs. ΔPG (156.46 ± 230.52), p = 0.0008] compared with PG.
Melatonin enhanced the GSH [ΔMG (10.51 ± 14.93) vs. ΔPG (₋5.05 ± 10.18), p = 0.004] and CHE2 levels [ΔMG (407.07 ± 723.26) vs. ΔPG (₋22.92 ± 506.52), p = 0.029] as well as sleep quality [scores: ΔMG (1.50 ± 1.28) vs. ΔPG (₋1.05 ± 2.05), p = 0.0006] and quantity [weighted total sleep time: ΔMG (0.74 ± 1.14) vs. ΔPG (₋1.04 ± 1.00), p = 0.0003] comparatively with placebo.
Caregivers may recommend 12-week nocturnal melatonin intake to attenuate cardiac autonomic dysfunction, oxidative stress and sleep disorders in MS patients.
Clinical registration This study was prospectively registered in the Pan African Clinical Trial Registry database (PACTR202007465309582) on 23 July 2020 (https://pactr.samrc.ac.za/.).
Graphical abstract
Highlights
• 12-week melatonin supplementation (3 mg per night) alleviated cardiac autonomic dysfunction (i.e., it increased heart rate variability) in multiple sclerosis patients.
• Exogenous melatonin had benefits on oxidative stress biomarkers (reduced glutathione, malondialdehyde and advanced oxidation protein products).
• Chronic nocturnal melatonin intake enhanced sleep quality, efficiency and quantity.