OrganicChilli
Senior Member (Voting Rights)
Abstract
Antibody-secreting cells (ASCs) play a central role in the pathophysiology of systemic lupus erythematosus (SLE). This single-arm, open-label, phase 2 clinical trial aims to evaluate the safety and efficacy of the ASC-depleting anti-CD38 monoclonal antibody daratumumab in patients with SLE (NCT04810754).
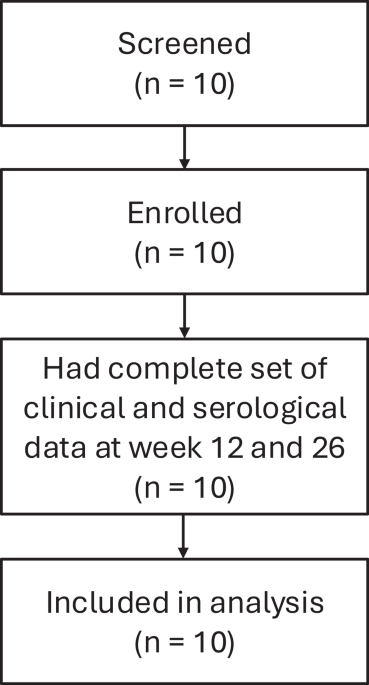
The primary endpoint is the reduction in serum anti-double-stranded DNA (anti-dsDNA) antibody levels at week 12. Key secondary end points include safety, clinical efficacy, and immunologic changes. Ten female patients with active disease and inadequate responses to at least two immunosuppressive drugs have received eight subcutaneous injections of 1800 mg daratumumab weekly, with dexamethasone as premedication (20 mg for first two injections, then 10 mg).
By week 12, anti-dsDNA antibody levels have been reduced by a median of 109.6 IU/ml (95% CI 38.1 – 274.5). The treatment resulted in rapid and sustained clinical improvements across all patients and organ domains, reflected by a 100% SRI-4 (Systemic Lupus Erythematosus Responder Index-4) response rate at week 12. Hypogammaglobulinemia occurred in 5/10 patients, requiring immunoglobulin substitution.
Daratumumab treatment has depleted circulating ASCs, reduced type I interferon activity, and profoundly modulated the T-cell responses. These findings highlight the pivotal role of ASCs in SLE pathogenesis and support daratumumab as therapeutic option for SLE.
 www.nature.com
www.nature.com
---
Median NK cell levels at baseline were 80 cells/µL as opposed to 153 cells/µL in the ME/CFS pilot study and they didn't seem to impact the outcome.
Antibody-secreting cells (ASCs) play a central role in the pathophysiology of systemic lupus erythematosus (SLE). This single-arm, open-label, phase 2 clinical trial aims to evaluate the safety and efficacy of the ASC-depleting anti-CD38 monoclonal antibody daratumumab in patients with SLE (NCT04810754).
The primary endpoint is the reduction in serum anti-double-stranded DNA (anti-dsDNA) antibody levels at week 12. Key secondary end points include safety, clinical efficacy, and immunologic changes. Ten female patients with active disease and inadequate responses to at least two immunosuppressive drugs have received eight subcutaneous injections of 1800 mg daratumumab weekly, with dexamethasone as premedication (20 mg for first two injections, then 10 mg).
By week 12, anti-dsDNA antibody levels have been reduced by a median of 109.6 IU/ml (95% CI 38.1 – 274.5). The treatment resulted in rapid and sustained clinical improvements across all patients and organ domains, reflected by a 100% SRI-4 (Systemic Lupus Erythematosus Responder Index-4) response rate at week 12. Hypogammaglobulinemia occurred in 5/10 patients, requiring immunoglobulin substitution.
Daratumumab treatment has depleted circulating ASCs, reduced type I interferon activity, and profoundly modulated the T-cell responses. These findings highlight the pivotal role of ASCs in SLE pathogenesis and support daratumumab as therapeutic option for SLE.
Daratumumab in systemic lupus erythematosus: a single-arm phase 2 trial - Nature Communications
CD38 is highly expressed by antibody-secreting cells (ASC) and depleting antibodies targeting CD38 have the potential to treat autoimmune diseases with ASC involvement. Here authors treat systemic lupus erythematosus patients with the ASC-depleting anti-CD38 monoclonal antibody daratumumab in...
www.nature.com
---
Median NK cell levels at baseline were 80 cells/µL as opposed to 153 cells/µL in the ME/CFS pilot study and they didn't seem to impact the outcome.
Last edited:
