You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
Deep phenotyping of post-infectious myalgic encephalomyelitis/chronic fatigue syndrome, 2024, Walitt et al
- Thread starter pooriepoor91
- Start date
Kitty
Senior Member (Voting Rights)
But, Nath said, the way he interprets the symptom based on what patients have said is that it's akin to having the flu and not wanting to get out of bed. "It's not like you're not capable of doing it, but your body tells you don't do it
ME patients and everybody who knows them and treats them can immediately see the error in this framing. Why is it so hard for doctors to explain that the signal can't be overridden, and "want" doesn't come into it?
I didn't "want" to have a thumping headache all day yesterday. I'm glad NIH didn't point out that my body is capable of not having a headache but it preferred to have one, because the only response that deserves is a high-velocity wet dishcloth.
So, the way I understand their symptoms, that's what's happening to these individuals. They got the infection, their body kind of shut down, and then it never recovered
Yet several years and eight million dollars later, you come up with "preference". We'll draw our own inferences about how much you understand.
Jonathan Edwards
Senior Member (Voting Rights)
"It's not like you're not capable of doing it, but your body tells you don't do it"
This is an awkward sentence for a start. I assume it would better be phrased with two 'thats'.
It's not that you're not capable of doing it, but that your body tells you don't do it.
This looks like it has been picked up from my comment to the Science journalist but it may just be the obvious analogy. But it is wrong and I am pretty sure not what I said.
It is that you, are not capable of doing it, with flu. Whether you refers to your whole organism or some putative 'mind' inside it isn't capable.
The inference that because muscles are working properly during short intensive exercise tests on a small maybe biased ME sample tells us nothing about the PEM that prevents people from leading a normal life. The people who could not even do the exercise tests are by definition selected out of the testing sample. For those that could, the flu situation arrives afterwards.
Maybe Dr Nath has not had Long Covid. If he had I find it hard to see how he can understand so little about the problem. Or at least about how to express his ideas.
This is an awkward sentence for a start. I assume it would better be phrased with two 'thats'.
It's not that you're not capable of doing it, but that your body tells you don't do it.
This looks like it has been picked up from my comment to the Science journalist but it may just be the obvious analogy. But it is wrong and I am pretty sure not what I said.
It is that you, are not capable of doing it, with flu. Whether you refers to your whole organism or some putative 'mind' inside it isn't capable.
The inference that because muscles are working properly during short intensive exercise tests on a small maybe biased ME sample tells us nothing about the PEM that prevents people from leading a normal life. The people who could not even do the exercise tests are by definition selected out of the testing sample. For those that could, the flu situation arrives afterwards.
Maybe Dr Nath has not had Long Covid. If he had I find it hard to see how he can understand so little about the problem. Or at least about how to express his ideas.
It is not entirely wrong, at least some of the time. I have had states where I could barely get across a room or to the toilet. But if the room had been on fire I could have done it, and quickly.But, Nath said, the way he interprets the symptom based on what patients have said is that it's akin to having the flu and not wanting to get out of bed. "It's not like you're not capable of doing it, but your body tells you don't do it…
The question is not can patients perform a single action, it is can they do it repeatedly, and without abnormally high cost?
That is just a brazen lie. What is the evidence for it?Both the autonomic and central motor dysfunction result in a reduction in physical activity. With time, the reduction in physical activity leads to muscular and cardiovascular deconditioning, and functional disability. All these features make up the PI-ME/CFS phenotype.
Last edited:
Is messing around with statistics, i.e. to get a significant result, not effort preference --- reward driven!Oh, dearie me!
A thread for the effort measure sounds a good idea. I would love to see conclusions but am unlikely to be able to follow the detail (even if because of lack of effort preference).
Trying to get something (anything) significant from 8 years & $8 million--effort preference!
hmm interestingNot sure whether this Medscape article by Mirian Tucker has been posted.
ME/CFS Experts Express 'Dismay' at Aspects of NIH Study
Miriam E. Tucker
February 28, 2024
She quotes comments from Bateman and Yellman and from Nath.
I thought this section from Nath was interesting (to put it politely) when responding to why they had used the term 'effort preference'
Quote:
According to Nath, "we battled around with ourselves about what is the right term to use. The problem is that it's a subjective sensation…And even the patients who experience it use a variety of different terms to describe it."
But, Nath said, the way he interprets the symptom based on what patients have said is that it's akin to having the flu and not wanting to get out of bed. "It's not like you're not capable of doing it, but your body tells you don't do it…Your body just wants to fight the infection. So, the way I understand their symptoms, that's what's happening to these individuals. They got the infection, their body kind of shut down, and then it never recovered…And we did find some of that reflected in their immune systems."
Dakota15
Senior Member (Voting Rights)
Yes, someone posted in the early pages of the thread that they had heard UCSF (I presume that's University of California at San Francisco?) was considering a trial.
Hopefully any universities considering trials might dig a bit deeper first rather than launching straight in - and they may have to, to get funding.
Just to be clear, I am neither pro-trial nor pro-viral-persistence-theory. My personal stance would be pro-more-digging into the "biological" findings in this and other studies to see which hold water, and then consideration of all the possibilities any that hold water could point to, followed by more digging.
I think premature trials could do more harm than good.
@Evergreen A few of us reached out to leaders at UCSF, and this intel was incorrect.
A few of us reached out to leaders at UCSF, and this intel was incorrect.
Like Peluso?
That explanation is complete BS. When you have the flu, the real flu, not a mild cold, there are things you certainly can do, like get out of bed to grab a glass of water, or answer the door, then probably forget that you even did that. But you certainly can't perform at work, cannot go out and socialize, cannot go for a run and do many things that are easy to do in every day life. You cannot perform regular activities of daily living, and it's not just about will, there is also there a very limited energy reserve that forces people to make choices that are simply not down to preference.Not sure whether this Medscape article by Mirian Tucker has been posted.
ME/CFS Experts Express 'Dismay' at Aspects of NIH Study
Miriam E. Tucker
February 28, 2024
She quotes comments from Bateman and Yellman and from Nath.
I thought this section from Nath was interesting (to put it politely) when responding to why they had used the term 'effort preference'
Quote:
According to Nath, "we battled around with ourselves about what is the right term to use. The problem is that it's a subjective sensation…And even the patients who experience it use a variety of different terms to describe it."
But, Nath said, the way he interprets the symptom based on what patients have said is that it's akin to having the flu and not wanting to get out of bed. "It's not like you're not capable of doing it, but your body tells you don't do it…Your body just wants to fight the infection. So, the way I understand their symptoms, that's what's happening to these individuals. They got the infection, their body kind of shut down, and then it never recovered…And we did find some of that reflected in their immune systems."
And that doesn't even take into consideration that a nasty flu with significant fever will definitely knock some people out to the point where they cannot even stand up, are so barely conscious that if you have a conversation with them afterward they will not even remember having. And how can "their body kind of shut down" be reconciled with "not like you're not capable of doing it"?
They struggled with the term but just happened to choose, to prefer, one that is exquisitely pejorative and highly suggestive of laziness? Horseshit.
Some posts have been moved to a new thread:
Use of EEfRT in the NIH study: Deep phenotyping of PI-ME/CFS, 2024, Walitt et al
To help navigation between the threads, links have been added to the first post in each thread. Please use the contact moderators button on any posts that you think have ended up on the wrong thread.
Use of EEfRT in the NIH study: Deep phenotyping of PI-ME/CFS, 2024, Walitt et al
To help navigation between the threads, links have been added to the first post in each thread. Please use the contact moderators button on any posts that you think have ended up on the wrong thread.
I was approached by journalists saying 'This looks like a damp squib that the science community is going to forget. But maybe an opportunity to flag up that ME is being taken seriously and some research is being done. Do you agree?' So I said yes and tried to think of something that ordinary people might connect to that was at least within the message of the paper.
After some further dialogue we all agreed that picking it apart would just make everyone miserable and maybe make enemies unnecessarily, for no real benefit so stick to plan A.
PACE was a major disaster that influenced care for a decade. This is not going to make any difference to what others do, I think. If Nath wants to try toxic drugs I am not sure how much that will have to do with the study. I rather suspect he will not have the courage.
Jonathan's (positive) post (above), read together with his positive comments here -
- https://www.s4me.info/threads/is-there-a-constant-anti-viral-response.37451/#post-518340 AND
- https://www.s4me.info/threads/uniqu...quences-2024-dunstan-et-al.37442/#post-518278
Suggest trying to get NIH to follow up the MRI study ("effort preference") with studies like those above (bullet points) i.e. looking for an underlying mechanism. The NIH ME/CFS Research Roadmap public consultation (closes 8th March) provides an opportunity to ask NIH to pursue this "sickness behaviour" hypothesis.
Last edited:
Super interesting thread from Todd Davenport about the anaerobic threshold differences between patients and volunteers, and how obviously different the demands from moderate activity are between the patients and controls. Something they seemed to have paid no attention to.
Well, since everyone's choosing their little part of the NIH Intramural Study to focus on, let's have a little "phun with physiology." Here's an interesting little factoid related to moderate physical activity as measured by actigraphy. Dang. So much disuse! Or is it?

The study considered moderate activity based on actigraphy data, rather than metabolic demand:I mean after all moderate activity is moderate activity, it isn't a big deal, and maybe people with PI-ME/CFS couldn't do it because they haven't done it. With their effort preference toward low value activities, maybe they didn't want to anyway. Right? Not so fast, my friends.
Here's this little factoid from the method section. Moderate physical activity is approximated as 3-6 times resting metabolism, which is defined as metabolic output from sitting down, which we also call a MET. So, this level of exertion is what we in the biz call "3-6 METs."
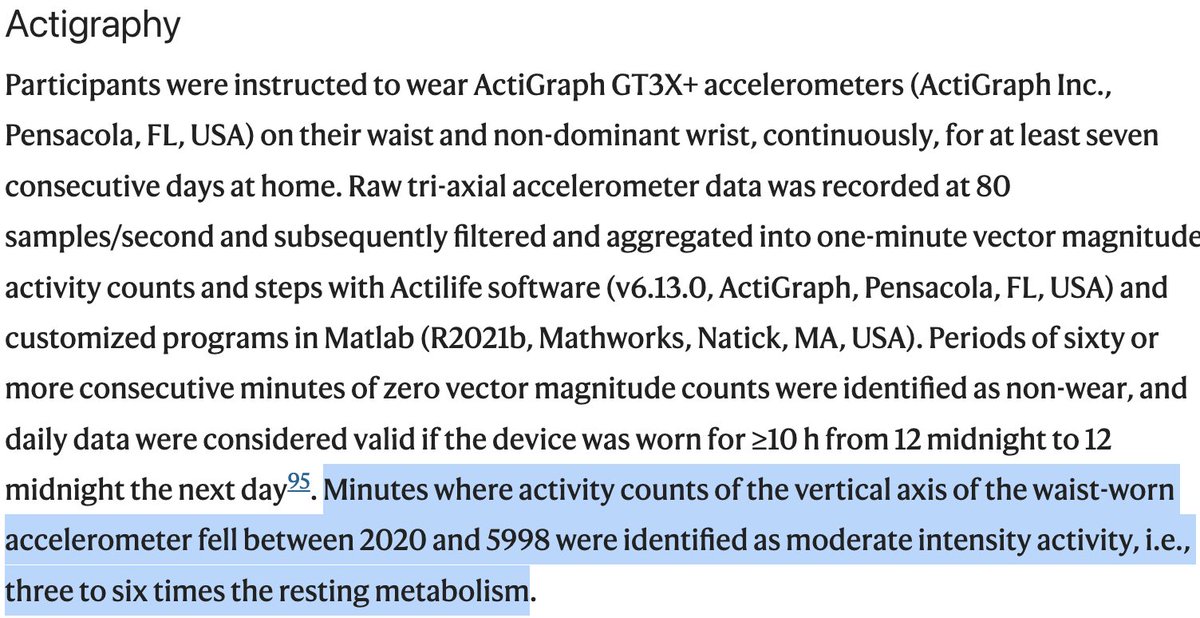
Does "moderate activity" turn out to be the same for all the participants? That would have been something a peer reviewer familiar with actigraphy and exercise testing would comment about before the article went to print. But it looks like that didn't happen. So what's the deal?
Ok, now let's flip back to Figure 5d, which are hella sciency looking boxplots showing peak VO2. The data is noisy, but the healthy volunteers performed, on average (middle bar in the box), at like 31ish ml/kg/min and the participants with PI-ME/CFS performed at 19ish ml/kg/min.
Bear in mind that that 1 MET is about 3.5 ml/kg/min. So we can work out the METs at peak exertion. For healthy volunteers, oxygen consumption at peak exertion was ~8.9 METs and for the participants with PI-ME/CFS it was 5.4 METs. But now wait a minute.
We said "moderate activity" was 3-6 METs. That means "moderate activity" was 34-67% of peak for healthy volunteers but 56-90% of peak for people with PI-ME/CFS. So, the same definition of "moderate," represents a very different metabolic demand between the groups. Just sayin'.
This is the meat:Don't believe me? You don't have to. Let's look at VO2 at anaerobic threshold, which is the physiological point past which physical activity becomes less sustainable. That point occurred around 16.5 ml/kg/min for healthy volunteers and 9 ml/kg/min (!!!) for people with PI-ME/CFS.
AT VO2 occurred at 4.7 METs for healthy volunteers, 2.6 METs for people with PI-ME/CFS. This means the definition of "moderate activity" on actigraphy was *above AT* for people with PI-ME/CFS. It was physiologically unsustainable. No wonder people with PI-ME/CFS did so much less.
And here's the thing. The authors undoubtedly left data on the table by not doing a two-day CPET, because AT likely may have been worse on the second day coinciding with symptoms, calling into question even more the "moderate" characterization of counts identified on actigraphy.
This is pretty much a demolition job.Super interesting thread from Todd Davenport about the anaerobic threshold differences between patients and volunteers, and how obviously different the demands from moderate activity are between the patients and controls. Something they seemed to have paid no attention to.
The study considered moderate activity based on actigraphy data, rather than metabolic demand:
This is the meat:
Todd Davenport should write a formal response to Nature
Boy, I'd think twice about using the word "behaviour" in any hypothesis that involves pwME with this group...The NIH ME/CFS Research Roadmap public consultation (closes 8th March) provides an opportunity to ask NIH to pursue this "sickness behaviour" hypothesis.
JemPD
Senior Member (Voting Rights)
Nath from Trish's post above said:"It's not like you're not capable of doing it, but your body tells you don't do it…Your body just wants to fight the infection. So, the way I understand their symptoms, that's what's happening to these individuals.
this was my thought exactly!ME patients and everybody who knows them and treats them can immediately see the error in this framing. Why is it so hard for doctors to explain that the signal can't be overridden, and "want" doesn't come into it?
I cant tell you the relief i feel when i read your posts illustrating that you get it. Thank you for listening, and hearing.The inference that because muscles are working properly during short intensive exercise tests on a small maybe biased ME sample tells us nothing about the PEM that prevents people from leading a normal life. The people who could not even do the exercise tests are by definition selected out of the testing sample. For those that could, the flu situation arrives afterwards.
So, re Todd’s thread, aside from the fact that NIH didn’t use it or report on this properly..
It’s interesting to me that quite a lot of metabolic dysfunction was found from a single day cpet, since proponents of the 2 day cpet tend to insist 2 days necessary to prove ME dysfunction. I know it gives more data to have two days, but, one day seems to provide very useful data and better in my view to subject people to less risk.
It’s interesting to me that quite a lot of metabolic dysfunction was found from a single day cpet, since proponents of the 2 day cpet tend to insist 2 days necessary to prove ME dysfunction. I know it gives more data to have two days, but, one day seems to provide very useful data and better in my view to subject people to less risk.
Peter T
Senior Member (Voting Rights)
So, re Todd’s thread, aside from the fact that NIH didn’t use it or report on this properly..
It’s interesting to me that quite a lot of metabolic dysfunction was found from a single day cpet, since proponents of the 2 day cpet tend to insist 2 days necessary to prove ME dysfunction. I know it gives more data to have two days, but, one day seems to provide very useful data and better in my view to subject people to less risk.
As I see it the issue is not that people with ME do or do not have issues with day one exertion, one would expect this is many conditions, rather what seems so far to be unique about ME is that previous exertion dramatically impacts on attempting day two exertion, so it would make sense to know what is going on on day two when people with ME have very distinct symptoms.
Obviously in this study people are exerting by just participating making it unclear what is day one and what is day two in real life, also any examination of ME metabolism may come up with interesting results, but on our current knowledge day two is the place we are most likely to find any pattern.
Andy
Senior Member (Voting rights)
Boy, I'd think twice about using the word "behaviour" in any hypothesis that involves pwME with this group...
- post-infection syndromes (used twice in the paper*)
- post-viral syndromes (used three times)
- adaptive sickness behaviours (used once)
- sickness behaviour or sickness behaviours (about 28 times)
*https://www.frontiersin.org/articles/10.3389/fncel.2024.1345441/full
Last edited: