Mij
Senior Member (Voting Rights)
Abstract
Long COVID (LC) is a multisystem condition that is linked to distinct pathologies including viral persistence, immunological dysfunction, endothelial damage, and mitochondrial dysfunction.
To date, limited research has assessed peripheral tissue hypoxia to better understand LC symptom exacerbation. Forty-six people with LC and 10 controls (CON) completed two submaximal cardiopulmonary exercise tests (CPETs), separated by 24-h. Near-infrared spectroscopy (NIRS)-derived signals from the left gastrocnemius muscle were continuously monitored before, during, and after 2-day incremental CPET.
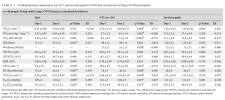
CPET outcomes demonstrated impaired physical function on day 2 compared with day 1 for the LC cohort at rest and VT1. LC tissue saturation index (TSI%) remained elevated above rest for a shorter duration of exercise compared to CON on day 1 (2nd minute vs. 5th minute).
On day 2, this response worsened for LC (Rest vs. 1st exercise minute: 63 ± 5% vs. 65 ± 5%; p < 0.05); meanwhile, CON exhibited sustained TSI% elevation throughout exercise above rest (Rest vs. 12th exercise minute: 62 ± 5% vs. 67 ± 4%; p < 0.05). LC TSI% remained elevated above rest for a shorter duration of exercise compared to CON, worsening for LC on day 2. LC showed rapid normalization of TSI%, suggesting impaired muscle oxygenation and recovery during repeated exercise.
Study
Long COVID (LC) is a multisystem condition that is linked to distinct pathologies including viral persistence, immunological dysfunction, endothelial damage, and mitochondrial dysfunction.
To date, limited research has assessed peripheral tissue hypoxia to better understand LC symptom exacerbation. Forty-six people with LC and 10 controls (CON) completed two submaximal cardiopulmonary exercise tests (CPETs), separated by 24-h. Near-infrared spectroscopy (NIRS)-derived signals from the left gastrocnemius muscle were continuously monitored before, during, and after 2-day incremental CPET.
CPET outcomes demonstrated impaired physical function on day 2 compared with day 1 for the LC cohort at rest and VT1. LC tissue saturation index (TSI%) remained elevated above rest for a shorter duration of exercise compared to CON on day 1 (2nd minute vs. 5th minute).
On day 2, this response worsened for LC (Rest vs. 1st exercise minute: 63 ± 5% vs. 65 ± 5%; p < 0.05); meanwhile, CON exhibited sustained TSI% elevation throughout exercise above rest (Rest vs. 12th exercise minute: 62 ± 5% vs. 67 ± 4%; p < 0.05). LC TSI% remained elevated above rest for a shorter duration of exercise compared to CON, worsening for LC on day 2. LC showed rapid normalization of TSI%, suggesting impaired muscle oxygenation and recovery during repeated exercise.
Study