[Initial public draft]
This model is not an attempt to capture every symptom that all patients experience, but is an attempt to explain the patient experience of what many patients see as being the core issue of ME, Post Exertional Malaise (PEM). It is also NOT an attempt to accurately explain what is happening biologically, it is merely an attempt to set out a logical description of the patient experience.
*******
Introduction
ME patients have both a reduced sustainable exertion limit, and an abnormal reaction to overexertion, both levels of which are individual to the patient and may change over time.
Sustainable exertion limit (SEL) is the maximum level of exertion that a patient can reliably replicate without overexerting. This is no different to a healthy person, who too will have a sustainable exertion limit, only for an ME patient this limit is considerably reduced.
For many patients it is not impossible for them to exert themselves above their SEL, however the question then is, what is their individual tolerance to overexertion at the time that they overexert.
Too much overexertion, that exceeds the individual patient's tolerance to it, without sufficient rest to counteract it, results in PEM. The severity of PEM is often closely related to the severity of a patient’s condition, as the lower a patient’s SEL is, the more likely it is that overexertion will accumulate.
This suggests that the mechanism in the body that, in healthy people, leads to increased fitness is, in some way, broken in ME patients. This also could be related to Delayed Onset Muscles Soreness (DOMS) which seems to share some elements of PEM.
Overexertion and/or PEM may be the main reasons why a patient’s condition might deteriorate over time, however there are reports from patients of declines despite avoiding overexertion to the best of their abilities.
Descriptions and explanations of ME patients mildly, moderately and severely affected, within the context of this model.
For descriptive purposes, the SEL of an average healthy person is assigned the ‘score’ of 100, and the average basal metabolic rate is scored at 30.
Note - no attempt has been made to align the mild/moderate/severe categories used here with any other scale used elsewhere. Also, it is not the intention to suggest that the categories used are distinct phenotypes, they are used for descriptive purposes only.
“Mild” sufferers
This description likely represents the majority of the patients that medical professionals will see. While their SEL has been reduced, through overexertion they may still be able to maintain much of their previous lifestyle. Typically this may present as working a typical week, but using weekends as rest periods in which they dramatically reduce their activity.
The activity of a mildly affected suffer might be represented by the chart below, where the patient’s activity during the working week is at 95, and at the weekend 75.
As long as the reduction in activity at the weekend is sufficient to counterbalance the overexertion during the week, this activity pattern might be long term sustainable.
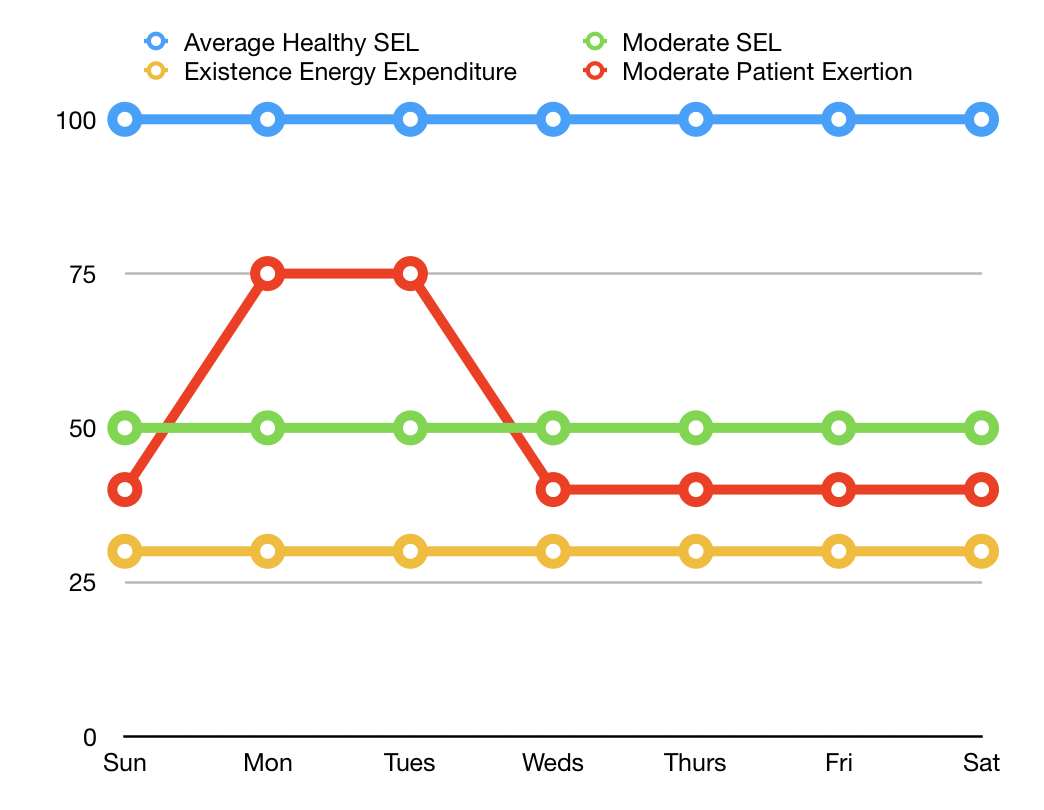
“Moderate” sufferers
This group will have made significant changes in their lives in order to maintain as much activity as is possible for them. They are unlikely to be working, almost certainly they won’t be working full time.
Here the patient, whose SEL is 50, has two days in which they exert themselves to a level of 75. In an attempt to recover/avoid PEM, they reduce their activity to a level of 40. Again, this activity pattern might be sustainable but, as can be seen, the patient’s life is dramatically limited.
“Severe” sufferers
[Note: I have a graph for this but didn't feel it added anything.]
Severe patients could well find themselves in a situation where the SEL is below their basal metabolic rate (i.e less than a score of 30 in this model). If this is the case, it would mean that they are in constant PEM, with no way of escaping from it.
End thoughts
One quirk of the above might explain the concept of why and how mild and severe sufferers might be in constant PEM, whereas moderate sufferers might be able to manage their exertion enough to avoid PEM altogether.
[End]
Comments and improvement suggestions welcome.
ETA: "End thoughts" paragraph added.