Abstract
Background
Previously, we reported a randomized placebo-controlled trial, the Qure study, showing that cognitive behavioural therapy (CBT), and not
doxycycline, was significantly more effective than placebo in reducing fatigue severity in
Q fever fatigue syndrome (QFS) patients. This follow-up study evaluates the long-term effect of these treatment regimens, 1 year after completion of the original trial.
Methods
All patients who completed the Qure study, CBT (
n = 50), doxycycline (
n = 52), and placebo (n = 52), were included in this follow-up study. Between twelve and fifteen months after end of treatment (EOT), patients filled out web-based questionnaires including the main outcome measure fatigue severity, assessed with the Checklist Individual Strength (CIS), subscale fatigue severity.
Results
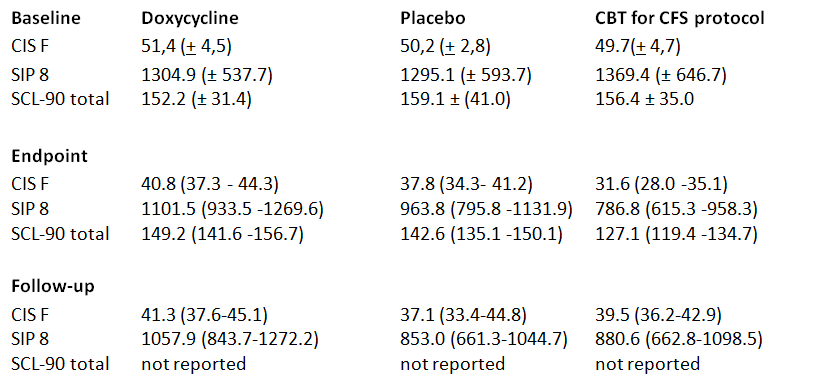
Fatigue severity in the CBT, but not doxycycline or placebo, group was significantly increased at follow-up compared to EOT (respective means 39.5 [95% CI, 36.2–42.9] and 31.3 [95% CI, 27.5–35.1], mean difference 8.2 [95% CI, 4.9–11.6];
P < .001). Fatigue severity scores of CBT (adjusted mean 39.8 [95% CI, 36.1–43.4]) and doxycycline (adjusted mean 41.0 [95% CI, 37.5–44.6]) groups did not significantly differ from the placebo group (adjusted mean 37.1 [95% CI, 33.6–40.7];
P = .92 and
P = .38, respectively).
Conclusion
The beneficial effect of CBT on fatigue severity at EOT was not maintained 1 year thereafter. Due to its initial beneficial effect and side effects of long-term doxycycline use, we still recommend CBT as treatment for QFS. We suggest further investigation on tailoring CBT more to QFS, possibly followed by booster sessions.