ME/CFS Science Blog
Senior Member (Voting Rights)
Looks like a decent study and analysis to me. The Twitter thread is quite useful for understanding the paper.
But unfortunate that they did not report the prevalence rate of ME/CFS.
They only note that "Among infected participants meeting criteria for ME/CFS, 98%met the criteria for PASC." More interesting would be to know which % of PASC patients meets ME/CFS criteria. I assume they have this information but prefer to keep this information for a separate paper?
I can't see anything in the paper that supports this statistic. Can anyone else?CNN article said:"Horwitz said that although most people in the study who met the definition of ME/CFS also met the definition of long Covid, the converse wasn’t necessarily true. Among people who met the definition of long Covid, only about 10% to 20% would have also met the definition of ME/CFS, meaning it may be an important subset of patients but isn’t exactly the same..."

I disagree with your premise. The RECOVER initiative may be producing results too slowly, but such an epidemiological characterization of long Covid is absolutely necessary and was long awaited. As the WHO’s poor definition of long Covid has proved, the quality of a case definition substantially impacts the quality of studies, from basic biological research to clinical trials. This is very welcome work, even though it is late, and it should definitely help with designing studies that will, in fine, serve to identify treatments.Disappointing, to be honest. It will not change anything, that's for sure, meaning we are no closer to any treatment for anyone.
I agree that it should. I just don't think that it will. I'm done with false hope.I disagree with your premise. The RECOVER initiative may be producing results too slowly, but such an epidemiological characterization of long Covid is absolutely necessary and was long awaited. As the WHO’s poor definition of long Covid has proved, the quality of a case definition substantially impacts the quality of studies, from basic biological research to clinical trials. This is very welcome work, even though it is late, and it should definitely help with designing studies that will, in fine, serve to identify treatments.
It hinges on whether researchers will adopt this definition of long Covid. Since it is operational (it comes with an easy-to-use score) and is based on a large scale and well done epidemiological study from the NIH, I am inclined to think that researchers will prefer it to the WHO’s vague definition and make the switch. The fact that the article was published in JAMA won’t hurt, either, but I understand your doubts.I agree that it should. I just don't think that it will. I'm done with false hope.
I can't see anything in the paper that supports this statistic. Can anyone else?
It's quoted in the CNN article. I'll amend my post to make that clear.Was it in a tweet or in comment somewhere by one of the authors? I thought I had seen it somewhere. However I am not on Twitter, so if it was a tweet I could only have seen it shared here.
The data is in Supplement 3.
On page 6
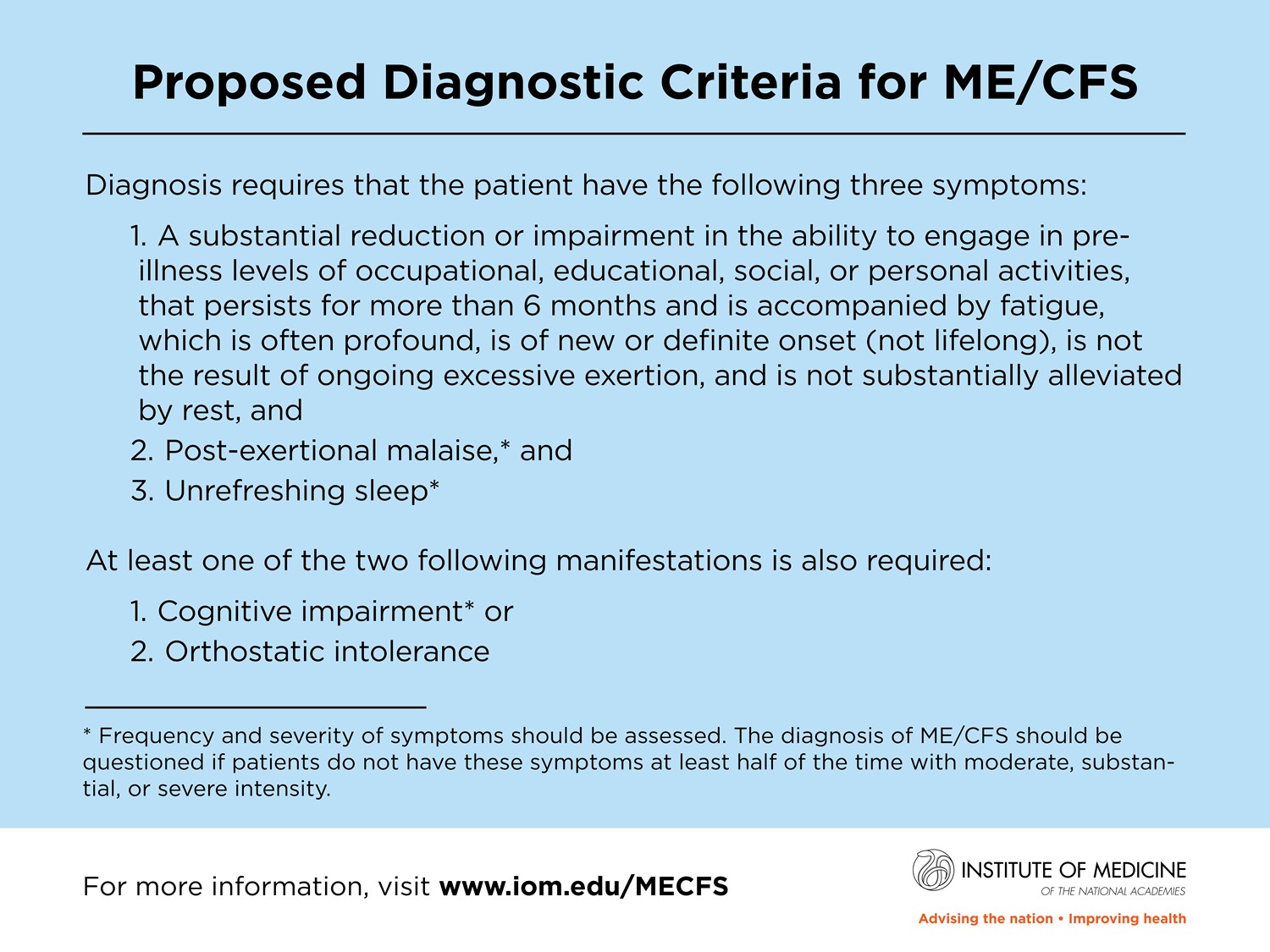
ME/CFS Definition
ME/CFS was identified using a definition based on the Institute of Medicine criteria. Participants were classified as having ME/CFS if they met all the following criteria:
A. Reported fatigue, reported severe or very severe fatigue on PROMIS Global-1071 Question 8, and had a PROMIS Global-10 physical health sub-score ≤10,
AND
B. Reported P-E Malaise,
AND
C. Reported Sleep disturbance and when asked “In the past 7 days, my sleep was refreshing”, the participant selected “Not at all”, “A little bit”, or “Somewhat”,
AND
D.
Either of the following:
a) Orthostatic intolerance (orthostatic tachycardia without orthostatic hypotension as obtained from the Active Standing Test)
OR
b) Reported brain fog and had a Neuro-QoL Cognition Score ≤40
My sleep pattern is pretty normal, so I wouldn't tick the box for 'sleep disturbance', even though I usually wake up feeling as though I have been run over.
Sleep is crucial for both high-level cognitive processing and also basic maintenance and restoration of physiological function. During human non-rapid eye movement (NREM) sleep, the electroencephalogram (EEG) exhibits low-frequency (<4 Hz) oscillatory dynamics that support memory and neural computation. In addition, functional magnetic resonance imaging (fMRI) studies measuring blood-oxygenation-level-dependent (BOLD) signals have demonstrated widespread hemodynamic alterations during NREM sleep.
Sleep is also associated with increased interstitial fluid volume and clearance of metabolic waste products into the CSF, and clearance is stronger in sleep with more low-frequency EEG oscillations. Why these diverse physiological processes co-occur within this state of low arousal is not known. In particular, it remains unclear how CSF dynamics change during sleep, and how they relate to the major changes in neural activity and hemodynamics.
We conclude that human sleep is associated with large coupled low-frequency oscillations in neuronal activity, blood oxygenation, and CSF flow. While electrophysiological slow waves are known to play important roles in cognition, our results suggest that they may also be linked to the physiologically restorative effects of sleep, as slow neural activity is followed by brainwide pulsations in blood volume and CSF flow.
These results address a key missing link in the neurophysiology of sleep. The macroscopic changes in CSF flow we identified are expected to alter waste clearance, as pulsatile fluid dynamics can increase mixing and diffusion. Neurovascular coupling has been proposed to contribute to clearance, but why it would cause higher clearance rates during sleep was not known. Our study suggests slow neural and hemodynamic oscillations as a new possible contributor to this process, in concert with other physiological factors.
Sarah Jolley said:@LisaAMcCorkell @myrabatchelder @katetwhitley @LesaSchultz143 The score is not meant for use clinically or to exclude individuals from long covid. It is a first step towards a definition that needs continued revision. It was important to get a summary out so that providers stop questioning and to guide next steps, but much still to be done.
In a recent JAMA article, researchers provided a new approach for identifying individuals with post-acute sequelae of SARS-CoV-2 (PASC), commonly referred to as long COVID. Because this article -- from Tanayott Thaweethai, PhD, and colleagues -- was part of the large, federally funded U.S. RECOVER study of long COVID, it will be influential among scientists around the world who are struggling with developing a case definition for long COVID. In this opinion piece, we suggest issues that might limit the interpretation of some of the study's findings -- in particular the identification of people who have long COVID.
In their introduction, Thaweethai and coauthors indicate that "Most existing PASC studies have focused on individual symptom frequency..." This is true, and it is a limitation in past studies, as either the "occurrence" of symptoms or just the "frequency" of symptoms are inadequate to help investigators understand the true burden of a post-viral symptom on a patient's life. Studies need to incorporate severity ratings into their scales. For example, some symptoms occur frequently, but their severity is so low that they may not burden the patient.
My concern is that the study from Thaweethai and colleagues still failed to broadly and sufficiently incorporate the "severity" measure, and used imprecise definitions and phrasing in some instances that may have skewed patient responses.