I may be well off the mark here and don't know the accuracy of these sources, but I did a quick search on MenACWY vaccination policies just to see if there were any trends that fit this data.
View attachment 31235
Norway noted that ages 16-19 may be a risk population due to graduation parties and travel, so recommends vaccination schedules to be completed right before this age:
The Norwegian Institute of Public Health recommends that young people aged 16-19 should consider vaccination against meningococcal disease.

www.helsenorge.no
Netherlands recommends for age 14:
The meningococcal vaccination protects against various meningococcal bacteria: types A, C, W and Y. That means it protects against meningitis and blood poisoning. Children receive this vaccination at 14 months and again at 14 years.

rijksvaccinatieprogramma.nl
Germany recommends for age 14 and again around college age:
Die Übersetzung des Originals des jeweiligen Aufklärungsblattes (Stand: 10/2025) erfolgte mit freundlicher Genehmigung des Deutschen Grünen Kreuzes e.V. im Auftrag des Robert Koch-Instituts. Maßgeblich ist der deutsche Text, für eventuelle Übersetzungsfehler kann keine Haftung übernommen werden...

www.rki.de
In the UK it's around 14 years old:
Find out about the MenACWY vaccine, including what it’s for, who should have it, how to get it and possible side effects.

www.nhs.uk
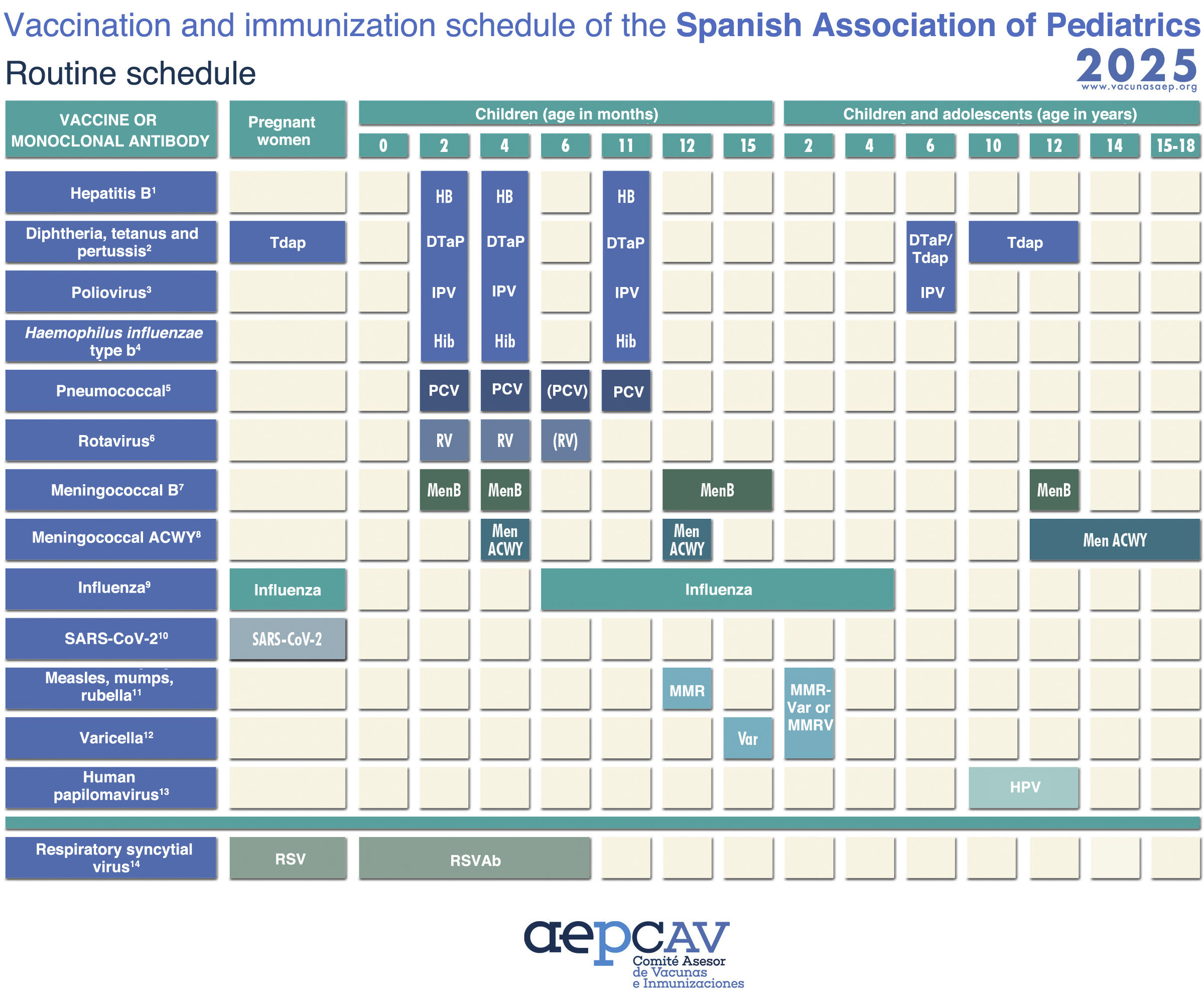
In contrast, Spain which had an almost non-existent early onset spike, recommends the MenACWY vaccine only in infancy:
The AEP 2025 Vaccination and Immunization Schedule recommended for children, adolescents and

www.analesdepediatria.org
France doesn't seem to neatly fall into the pattern, though. It didn't have the strongest early peak, and it recommends the vaccine between 11-14:
Vaccination schedule: what changes for 2026?

www.service-public.gouv.fr
Couple caveats: policies may have changed in recent decades so these sources might not reflect the reality of the people responding to the survey. This is also only for MenACWY--it seems like countries have different recommendations for menB boosters as well (Spain, for instance, recommends MenB boosters at 12)
Might be nothing relevant here but I just thought it would be interesting to check, especially since actual meningitis presents with sensory sensitivities similar to severe ME/CFS. LPS can trigger a neuroimmune "sickness behavior" response, so I thought a bacterial vaccine might be able to as well and might tie into some epigenetic mechanisms we've been discussing elsewhere. Or I could just be hallucinating a pattern where there is none.