I am glad I saw this thread. I will share my experience (ongoing) in case it might help others or provide any clues:
I've also noticed unusual dry mouth/thirst and nocturia developed alongside the typical symptoms of me/cfs. It's not severe, just another annoyance and possible piece of the puzzle.
This is how it started for me as well. Like everything with my ME/CFS though, it continued to progress. If anyone is experiencing these symptoms, consider tracking fluid intake/output for a few days, and maybe catch it earlier than I did. Finally a 24-hr urine test for something else in which I collected an excessive volume, and could prove it was far less than the volume I had consumed, convinced my primary doctor to make an endocrinology referral.
Has anyone here been diagnosed with Diabetes Insipidus or has been prescribed Desmopressin and had response for their symptoms?
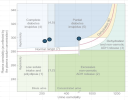
I have been diagnosed with partial central DI, (
Arginine vasopressin deficiency, AVP-D). A plot with my osmolality values are attached. Copeptin/ADH were present, but low.
My understanding is that in the absence of a pituitary tumor or traumatic brain injury, other idiopathic cases of Central DI are considered to be immune/infection/inflammation, or autoimmune-driven. The endocrinologist called it "Lymphocytic infundibulo-neurohypophysitis.
" (
Diagnosis and Management of Central Diabetes Insipidus in Adults, 2022) There is an antibody,
anti-rabphilin-3A, that is being studied in this context, but as far as I can tell it is not used clinically yet. (my endocrinologist knew about it, but did not have a way to order it)
I started Desmopressin (DDAVP) about 6 weeks ago. My endocrinologist is having me slowly titrate up and drawing labs every week to monitor for hyponatremia.
What has improved:
- Less thirst and polyuria/nocturia
- Fewer PVC / skipped beats (perhaps blood volume increasing?)
What has not improved:
- All other ME/CFS symptoms (activity threshold, ability to recover from minor exertion, sleep quality, etc.)
- Tachycardia (but as I have said in other threads, mine seems to be "exertional" not "positional"/POT)
Random thoughts about other puzzle pieces:
- I had echocardiograms ~6 months apart. The cardiologist who reviewed the second one said "Your heart has shrunk 20%." .. Was this a compensation for low blood volume? Or some other ME process?
- Vasopressin has other functions in the body (vasoconstriction, glycogen breakdown, ACTH secretion, circadian rhythm, cognition and emotion) and there are multiple AVP receptors. (
Wikipedia) DDAVP only acts on the V2 receptor, which allows water to be reabsorbed. It does not act on the other receptors. So, if AVP deficiency is contributing to other symptoms, DDAVP will not help.