ryanc97
Senior Member (Voting Rights)
what is your take on the wording? does it imply the levels are similar or constant?Suggestive.
what is your take on the wording? does it imply the levels are similar or constant?Suggestive.
Don't know about the other antibodies but I'm pretty sure we've seen studies showing some fluctuating test results for the SARS-COV-2 antibodies including some decay over time. Given the duration of study an asymptomatic infection might also not be completely unlikely in a small subset of participants. So I would naively think "similar" levels is the best one could expect.what is your take on the wording? does it imply the levels are similar or constant?
Can’t antibodies persist in the blood for a while even if the cells that produced them are no longer there?
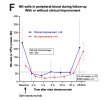
For the seven shot cohort, IGG didn’t decrease with the 3 additional shots (the yellow arrows). Any ideas about this? Maybe Daratumumab can’t deplete any more cells without NK cells?
Just now noticing that the NK cell count of the responders went up to baseline levels.
Presumably that means that NK count by itself is not a useful indicator of severity, because then you’d expect relapses as soon as NK cell counts normalised.
It could still be possible that disease severity was mediated by some specific type of NK cells that didn’t get repopulated in the responders?
——
I also see that almost all of the non-responders ended up with higher NK cell counts, and most of them above the responder-threshold.
Did they try giving those more Dara, and do we have data on it?
I wonder why not? maybe it's so as not to dilute the evidence in favour of dara if it doesn't work but surely if they now have counts above the threshold it would give a clear indication whether there is a direct relation between NK cells and response or something more complex.They are not planning to retreat non-responders, but they will retreat responders if and when they relapse.
Isn’t it normal in cancer research to specifically study pre-treated patients?I wonder why not? maybe it's so as not to dilute the evidence in favour of dara if it doesn't work but surely if they now have counts above the threshold it would give a clear indication whether there is a direct relation between NK cells and response or something more complex.
I find this decision frustrating, even if I can see why its been made.
Maybe yeah. I just think it's a shame that they're not going to retreat the non responders who now have higher NK cells because we could get some idea of whether the relationship between response and NK cells is as simple as how many you have.Isn’t it normal in cancer research to specifically study pre-treated patients?
Like they tried X, Y and Z that are the preferred treatments, and now we’re trying T for the people that still need it?
Maybe we’ll get that down the line if Dara works.
It would be unblinded and they have limited funding, so that might be the reason for using the doses where it can get the most robust data.Maybe yeah. I just think it's a shame that they're not going to retreat the non responders who now have higher NK cells because we could get some idea of whether the relationship between response and NK cells is as simple as how many you have.
It feels frustrating to potentially wait years to find out when they could start looking into it now.
Agreed that would be interestingIt would also nice to have data to see if artificially boosting NK cell count makes any difference, and if the types of NK cells matters.
Lets hope so!I hope the Germans do some of this with their studies that have pharma funds.
Me too. I'm trying to be realistic and temper my hopes but this seems really promising and it's quite hard to stay level headed about it.I do really hope the responses are genuine it will/would be disappointing if the rct doesnt show any effect.
I wonder why not? maybe it's so as not to dilute the evidence in favour of dara if it doesn't work but surely if they now have counts above the threshold it would give a clear indication whether there is a direct relation between NK cells and response or something more complex.
All good points.If they didn't respond first time, it's reasonably likely they won't respond next time. The drug is expensive and not without risk, so there may be an ethical argument against it at this stage.
Until they've made progress on understanding whether it works, and if so why, they have to tread carefully. Should the trials suggest strongly that it's a viable treatment for some, they can then start thinking about alternatives for non-responders. It's possible that group needs a different drug, or a combination of drugs, or to boost their NK counts beforehand, or that they have a different disease needing an entirely different approach. It seems likely the latter will be the case with a proportion of people with ME/CFS, even if it's only a small one.
At this point my hunch is that the cell count indicates the dysfunction level as well. So you really need a high count or boosted NK cells to get something out of Dara.All good points.
I just feel that if they took this group of 4 non responders, if their NK cell counts are now over the threshold as Utsikt says, and retreated them and followed them as a case study as with these low dose patients they did recently and the severe patients they will do next year, it would give a small but valuble indication of whether increasing NK cells would turn non responders into responders (in at least some cases).
Be careful about boosting NK-cells.At this point my hunch is that the cell count indicates the dysfunction level as well. So you really need a high count or boosted NK cells to get something out of Dara.
To me this is the case because the doses are small compared to MM dosing where they can do like weekly Dara over the course of 6 months. So in theory the NK cell effect might be more important because of the small dose whereas in MM the amount of Dara thrown at the patient just ends up working.
What makes it even worse is that Covid has shown to impact lymphocyte function. So those with repeated Covid infections in the trial probably might have poor NK cell function overall despite enough counts. And that could confound things.
Now if only they decided to boost NK cells via Anktiva for patients before giving them Dara....
Be careful about boosting NK-cells.
I think I don't get the flu-like symptoms when in PEM because of low NK-cells.
I won't try boosting the cells unless it is proven to be helpful; if and when treatment becomes available.
 that would explain why IGG drop between non responders and responders max difference was like 10-15%.
that would explain why IGG drop between non responders and responders max difference was like 10-15%.