The term “chronic fatigue syndrome” names a psychiatric condition that sometimes develops in reaction to acute viral infection.[2] [3] [4] It is essentially deconditioning that arises from inactivity when patients embrace faulty illness beliefs.
By contrast, the term “myalgic encephalomyelitis” or “ME/CFS” names a chronic biomedical disease that typically develops after acute viral infection.[5] [6]
However much many of us might dislike the term "chronic fatigue syndrome" and would like to see it deprecated, it remains the fact that NHS England mandates the use of SNOMED CT terminology system and ICD-10 classification and codes for its Data Sets.
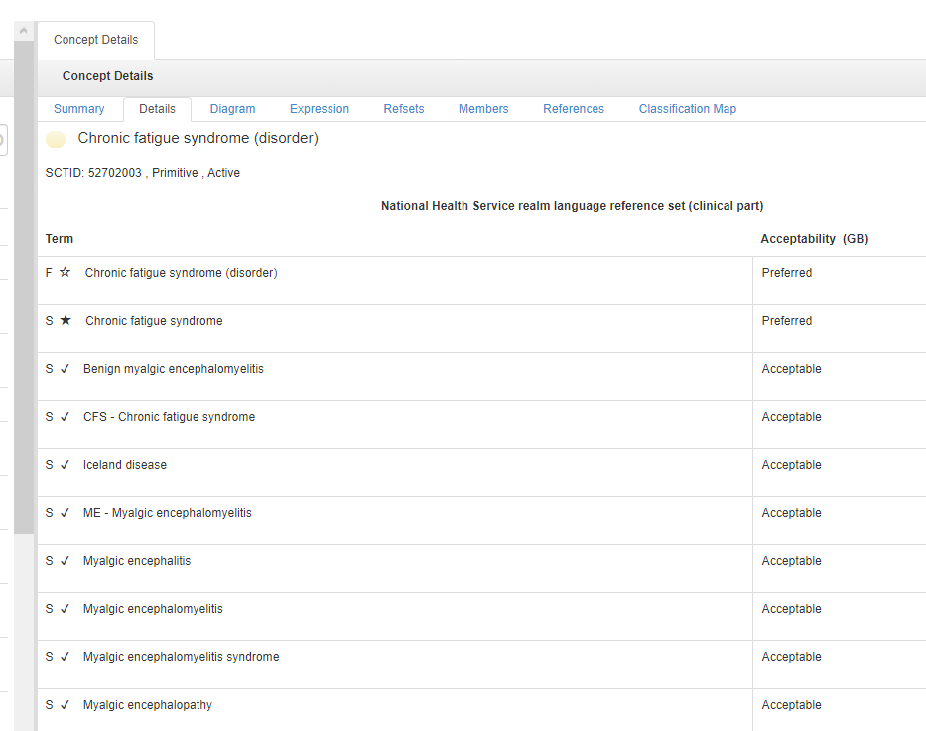
1 SNOMED CT, the mandatory terminology system for use across NHS England primary and secondary care settings, at the point of care, uses "Chronic fatigue syndrome" as the "Fully Specified Name" and "Preferred" term and cross maps Concept code SCTID
52702003 | Chronic fatigue syndrome and all the terms listed under Synonyms, to
ICD-10 G93.3:
SNOMED CT UK Edition:
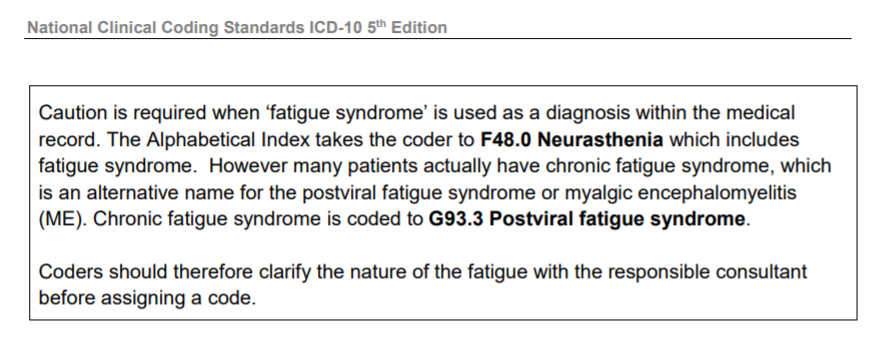
2 The annual publication: NHS Digital National Clinical Coding Standards ICD-10 has included this note for coders for a number of years:
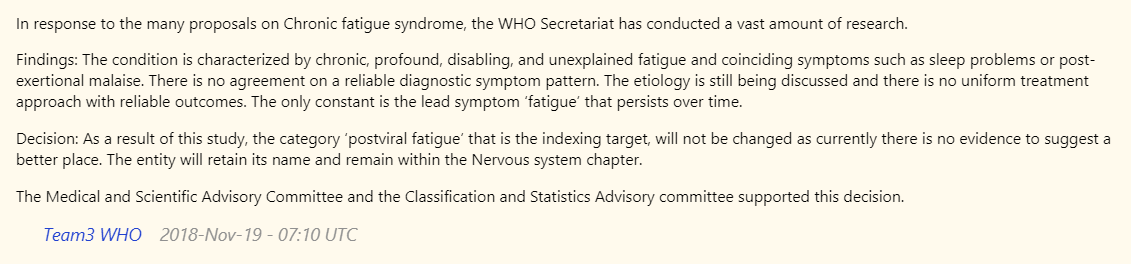
3 The WHO's statement (published November 19, 2018) regarding classification for the forthcoming ICD-11 of 8E49 Postviral fatigue syndrome and its inclusions: 8E49 Benign myalgic encephalomyelitis and 8E49 Chronic fatigue syndrome:
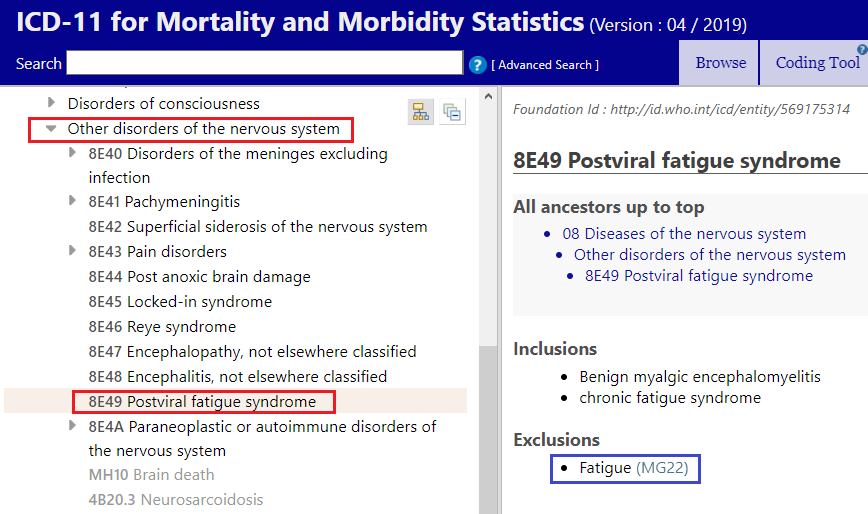
4 8E49 Postviral fatigue syndrome and its inclusions 8E49 Benign myalgic encephalomyelitis: and 8E49 Chronic fatigue syndrome for ICD-11:
5 In one of her recent papers, O'Leary has referenced that the WHO recently accepted and implemented my proposal that all three terms:
8E49 Postviral fatigue syndrome;
8E49 Benign myalgic encephalomyelitis;
8E49 Chronic fatigue syndrome
should be specified as Exclusions under ICD-11's
Chapter 06 Mental, behavioural or neurodevelopmental disorders category:
6C20 Bodily distress disorder.
The convention for both SNOMED CT terminology system and for ICD is not to classify conjoined terms, eg "CFS/ME" or "ME/CFS".
Both systems classify a
"Fully Specified Name/Preferred term" (in the case of SNOMED CT) and a
"Concept Title" term (in the case of ICD), under which alternative terms are listed as
Synonyms terms or as
Specified Inclusion terms. (Or in the case of Chronic fatigue syndrome in the international edition of ICD-10, included in the
Index and indexed to the target code, G93.3).
Therefore, whatever terminology the clinician, coder or admin staff enters manually into the primary care patient electronic medical record (EMR) system or into the secondary care EMR, all three discrete terms will be recognised and all cross mapped or coded to ICD-10 G93.3 (or to 8E49, when ICD-11 has been implemented).
And that will be the case with "Chronic fatigue syndrome", whichever acronym NICE might decide to take forward for use in its forthcoming revised guideline.
Please consider how helpful it is to have Dr O'Leary asserting:
The term “chronic fatigue syndrome” names a psychiatric condition that sometimes develops in reaction to acute viral infection.[2] [3] [4] It is essentially deconditioning that arises from inactivity when patients embrace faulty illness beliefs.
By contrast, the term “myalgic encephalomyelitis” or “ME/CFS” names a chronic biomedical disease that typically develops after acute viral infection.[5] [6]...While CFS is a condition we can hope to resolve with holistic virus recovery strategies...
So no, I don't find it of interest; I find it unhelpful and potentially confusing to clinicians and coders working in NHS England primary care and secondary care who will continue to code patients in electronic medical records and will continue submitting data to local NHS Trusts, to NHS Digital, NHS England and the WHO, using two mandatory terminology and classification systems that map and code
all three terms to ICD-10 G93.3 in the
Diseases of the nervous system chapter, and in the case of the mandatory SNOMED CT UK Edition, specifies Concept code SCTID
52702003 | Chronic fatigue syndrome as the
"Fully Specified Name/Preferred term".
Edited to add:
Three more Rapid Responses to the BMJ Practice Pointer: Management of post-acute covid-19 in primary care that refer to CFS, CFS/ME, ME/CFS, ME, PVFS, classification and coding:
From
Andrea D Martell, 28 August 2020:
https://www.bmj.com/content/370/bmj.m3026/rr-5
Dear Editor, I would like to object to Dr. O'Leary categorizing Chronic Fatigue Syndrome as a psychiatric condition...
From
Arvind Joshi, Physician (Medicine and Therapeutics), Mumbai, 14 August 2020
https://bmj.com/content/370/bmj.m3026/rr-1
From
Colin D Watt, Retired, North Berwick, Scotland, 14 August 2020
https://bmj.com/content/370/bmj.m3026/rr-0
------------------------------------------------------------------------------------------
Edited to add:
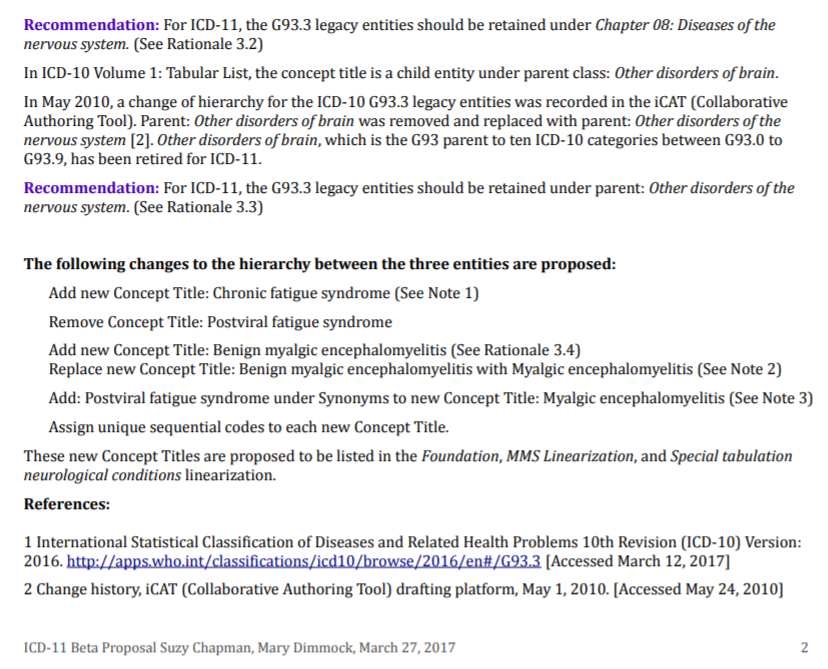
Proposal and rationale submitted to ICD-11 Proposal Platform by Chapman & Dimmock, March 27, 2017: http://bit.ly/2mQxWTS
Our proposal recommended creating a new Concept Title code for Benign myalgic encephalomyelitis and a new Concept Title code for Chronic fatigue syndrome, and assigning discrete sequential codes for each new Concept Title.
Assigning discrete codes for these two terms was rejected by the WHO in November 2018.
Extract p2:
Download my August 2020 report:
Update on classification and coding of PVFS, ME and CFS for ICD-11 here:
https://dxrevisionwatch.files.wordp...ion-of-pvfs-me-cfs-for-icd-11-august-2020.pdf