In reality, the crux of the issue is surely this:
I don't think it's as clear cut as that. That study appears to have done CPET studies on a number of male patients over a period of time. The CPETs were part of a diagnostic process, which classed people as having ME/CFS or not. I think it's highly likely that anyone having a positive CPET test would be assessed as having PEM, and the fact that they are in the clinic means they have fatigue. So probably all of the people with a positive CPET got the label 'ME/CFS', and the people with a negative CPET got the label 'ICF'. The researchers did not actually do new CPETS, so we don't know how replicable CPETs are. (We need studies on that.)
It's very possible that some of the people showing a good response to exercise in the paired CPETs were just having a good period in their illness. Perhaps their trigger for PEM was higher than 8 minutes on a bicycle. Perhaps some of them were really well rested before the test and some of them weren't.
So, it's quite likely that people with a positive CPET in this clinic were classed as having ME/CFS. And so when charting the results of the people diagnosed with ME/CFS and people diagnosed as without ME/CFS, it is hardly surprising that the people with ME/CFS are found to have a positive CPET. It's circular.
edit: link to the discussion thread on this paper
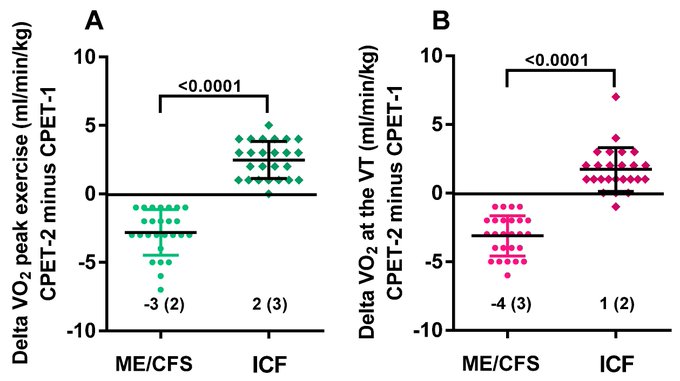
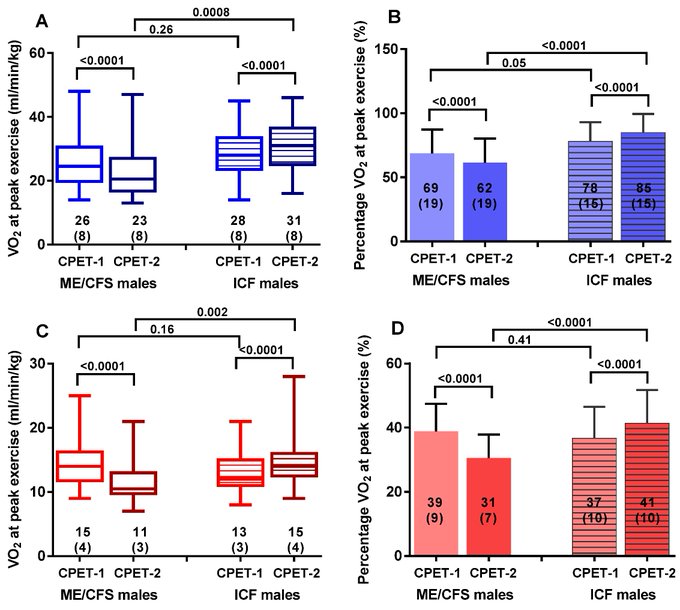
Comparing Idiopathic Chronic Fatigue and ME/CFS in Males: Response to Two-Day CPET, 2021, van Campen and Visser
Trials with mixtures of people with fatigue meeting and not meeting criteria requiring PEM have not shown GET is helpful. Why could that be?
One possibility is that processes for assigning people to various criteria aren't very good. It might be hard to know if you have PEM, if no one describes it to you well, or if your life is not very regimented, so that it's hard to see patterns. The doctor asking the questions might just have been really useless. So some of the people who are recorded as not meeting more stringent criteria might actually get PEM, and might really have ME/CFS.
Another possibility is that graded exercise therapy isn't helpful in more fatiguing conditions than just ME/CFS.
Another possibility is related to the fact that the efficacy of GET relies on two assumptions - one is that exercise really does improve the health condition. The second is that telling someone that they need to exercise more actually makes them exercise more. So, even if, in theory, exercise could make some of the people with fatigue feel better, if telling them to exercise doesn't make them exercise more, then telling them to exercise is not a useful treatment.
Another possibility is that GET artificially reduces the amount of exercise a person is doing to start with - to establish the baseline before gradually increasing it. The end result might therefore be some people feeling a bit better initially because of less activity and then feeling as bad as ever as the level of activity goes back to what it was. But, overall, the amount of exercise the participants do doesn't change from trial start date, and so even the people who might benefit from exercise don't experience a benefit.