As part of our Values and Policy process, #MEAction designed a survey regarding the diagnostic criteria for ME, ME/cfs, and CFS; we then sent that survey to clinicians who treat or have treated pwME as their main patient population, and researchers who study ME as one of their main areas of focus. We contacted 65 researchers and clinicians, receiving 22 completed survey questionnaires and four sets of stand-alone comments via email. No biopsychosocial (BPS) theorists or clinicians, who view the disease as treatable via changes in behavior, were contacted.
Read the full survey results here.
The Canadian Consensus Criteria was judged best definition for research and clinical use, for both specialist and mainstream medical practitioners.
Though some questions required a definitive answer, while in others, responders were able to choose multiple sets of criteria, the most popular responses for every question about criteria were, in order:
1. Canadian Consensus Criteria (CCC)
2. National Academies of Medicine / Institute of Medicine criteria (NAM/IOM)
3. International Consensus Criteria (ICC)
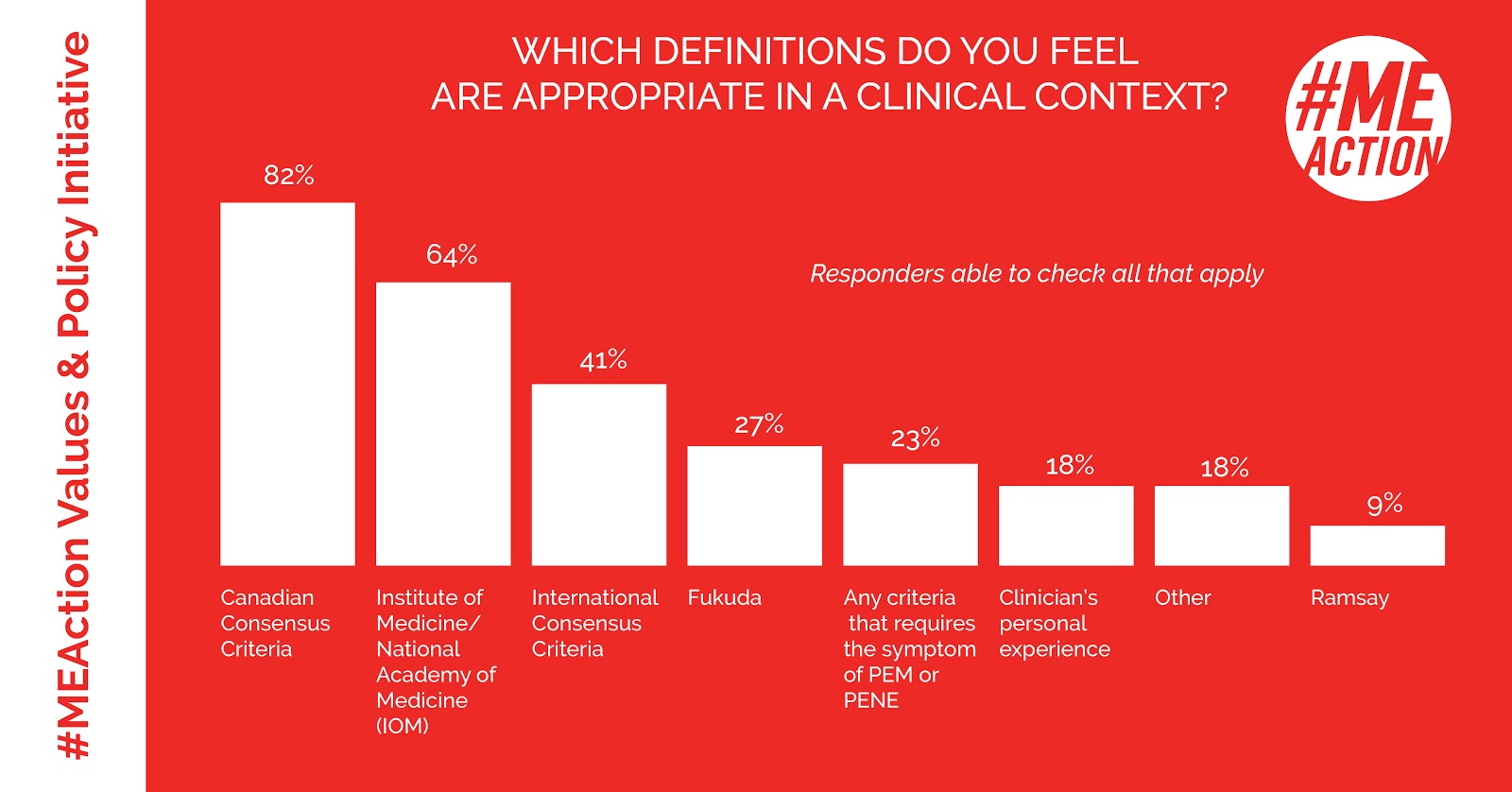
Which definitions are appropriate?
There were significant gaps between the popularity of the responses. For example,
82% of responders agreed that CCC is appropriate for clinical use, including
100% of clinicians surveyed.
64% considered NAM/IOM appropriate for clinical use, and
41% agreed ICC is appropriate for clinical use. Note that responders could choose as many answers as they thought were appropriate.
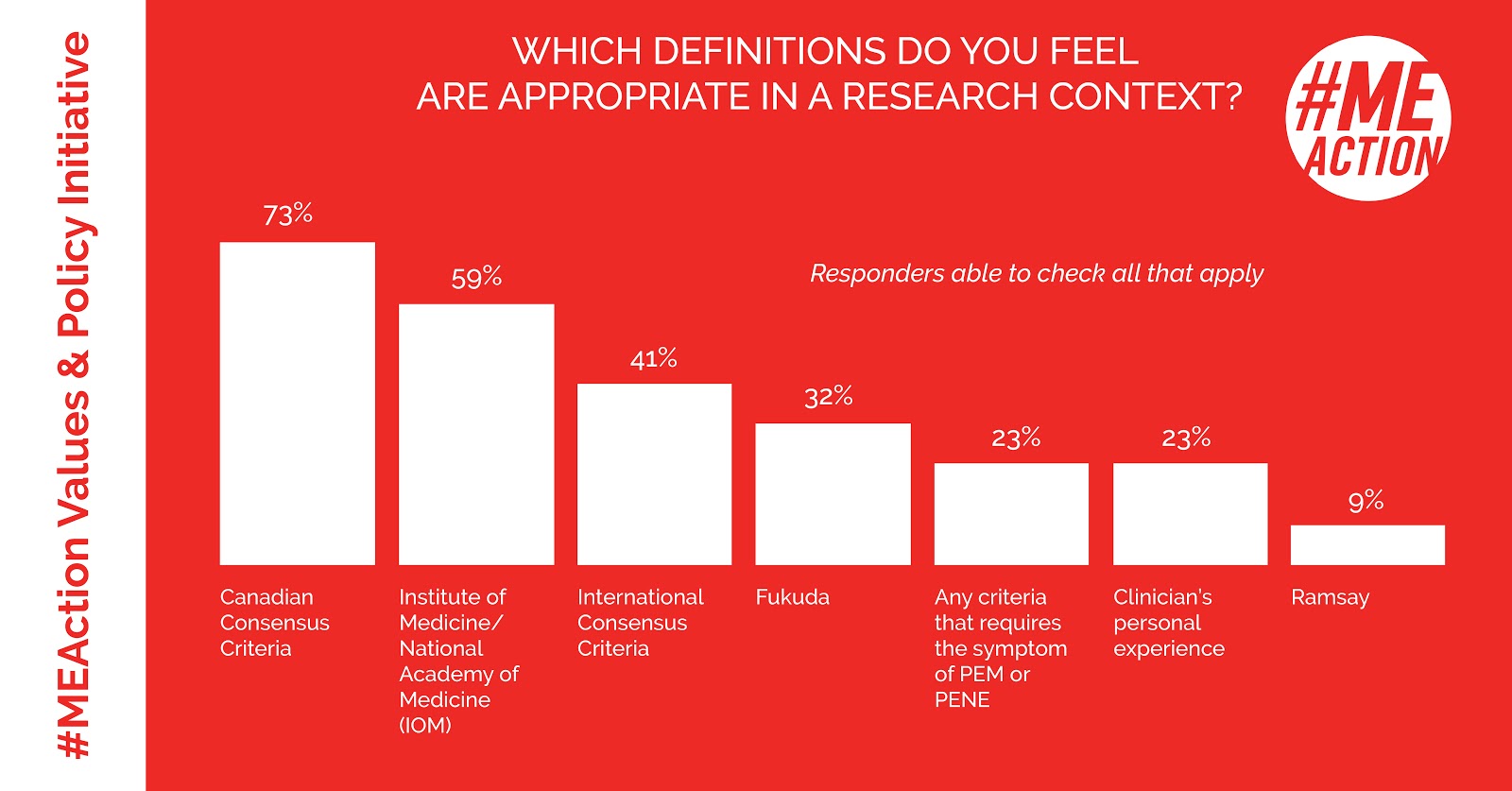
When responders were asked which criteria were appropriate in a
research context, once again the
Canadian Consensus Criteria led, with the gap closing between CCC and the IOM/NAM set of criteria. Once again, responders could choose as many criteria as they considered appropriate for research use.
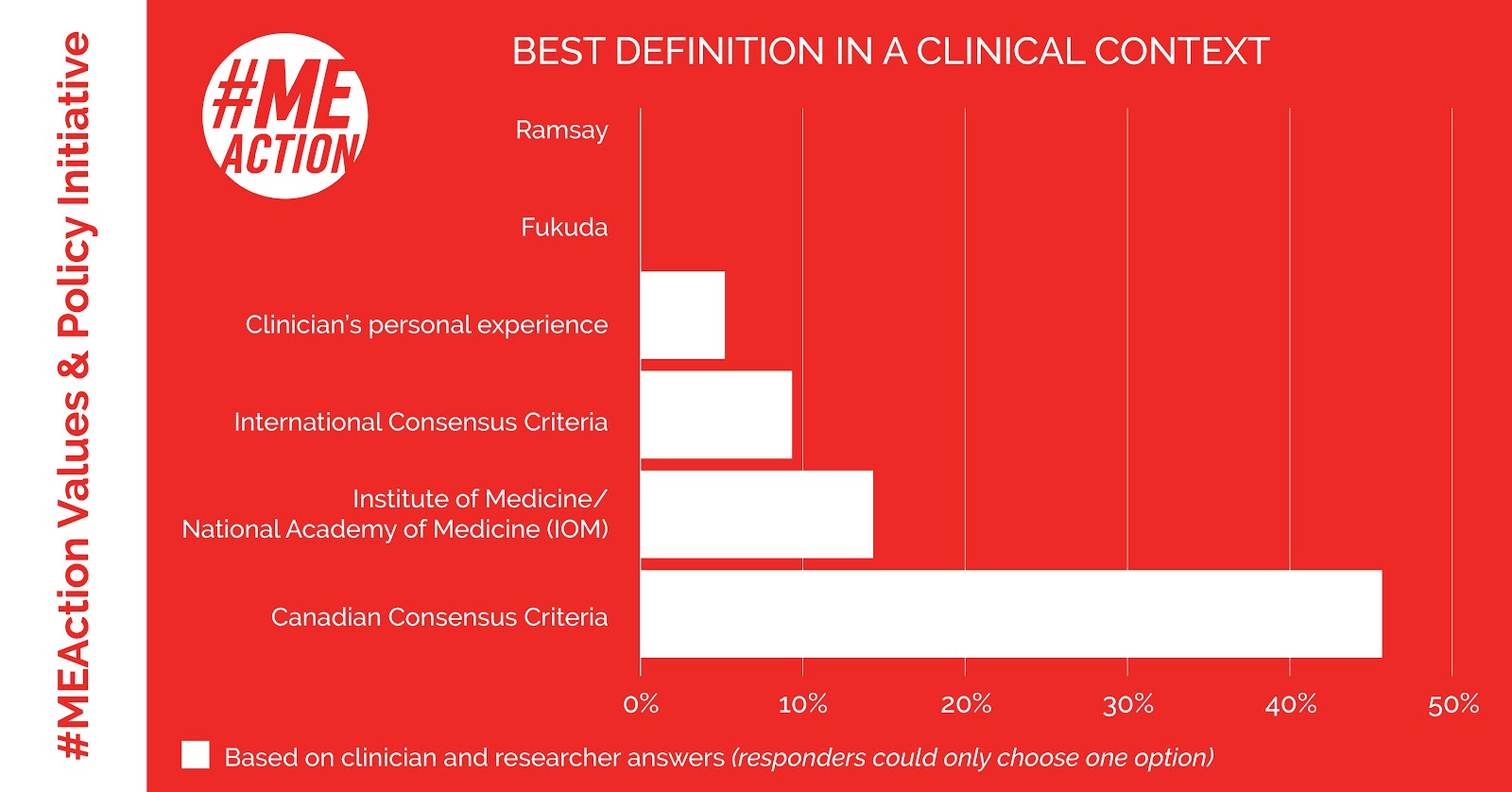
Which definitions are best?
When asked which set of criteria was
best suited to clinical use and only able to choose one answer, once again, the
Canadian Consensus Criteria (CCC) came out far ahead of the other potential choices. The
Institute of Medicine criteria came in a distant second.
When asked to choose
only one set of criteria for research, the numbers were much the same:
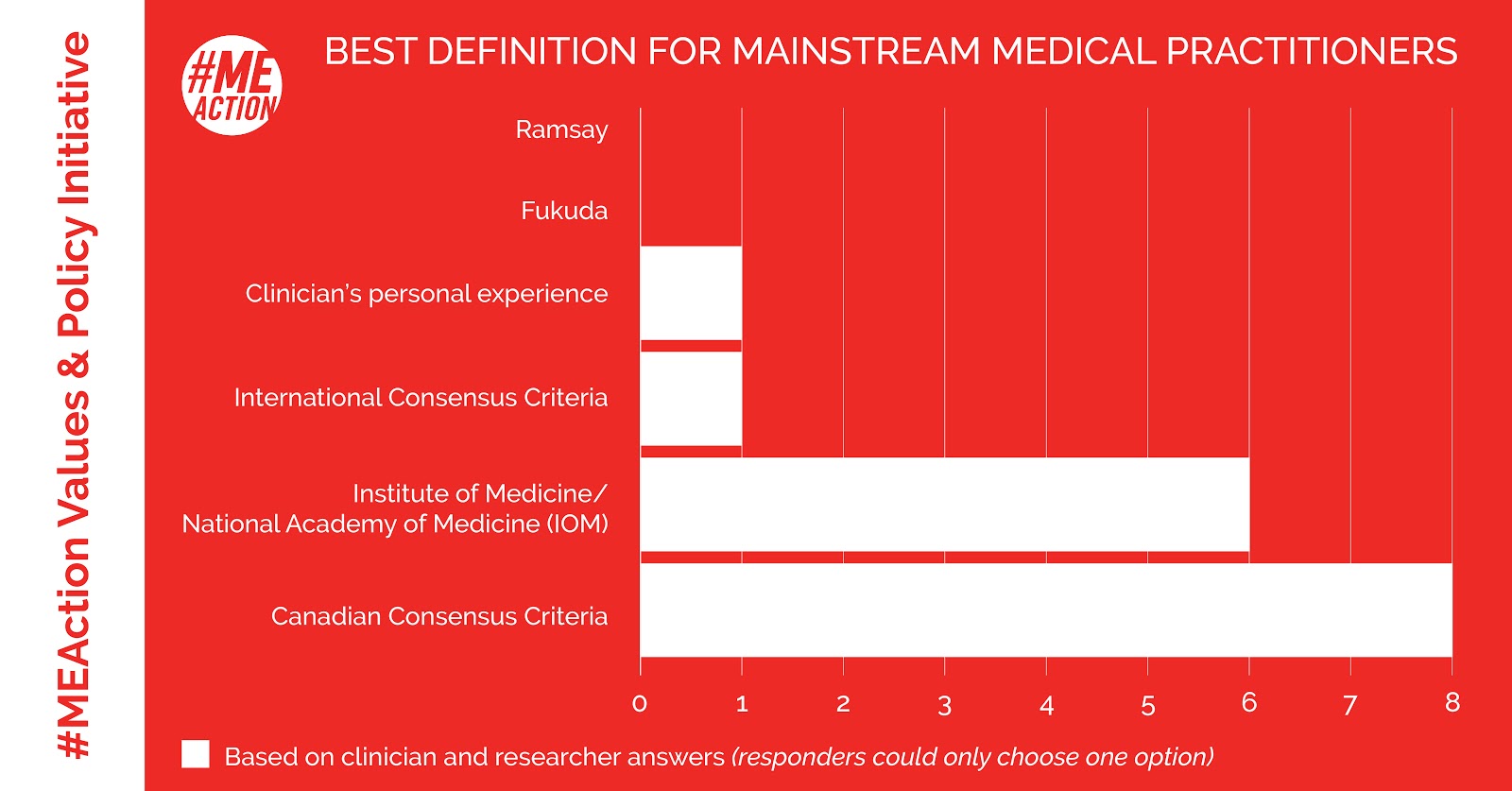
When responders were asked which set of criteria was
best for mainstream medical practitioners, the
gap between CCC and IOM/NAM closed significantly, but the order remained the same:
Why did ME-literate researchers and clinicians consistently choose the Canadian Consensus Criteria?
In their own words:
“Often [in] some patients either cognition, pain or sleep is not affected - so the
Canadian criteria has more flexibility to include these patients.”
“CCC
best defines all the presenting aspects of illness. The
IOM criteria are more straightforward, good for screening using the core symptoms, are
evidence-based and
widely available to all practicing clinicians.”
“
IOM is a simplified version of CCC: a way to get a GP to recognize the disease when they see it and refer out to a specialist.
CCC captures a specific cohort and
has the four required symptoms of fatigue, PEM, sleep dysfunction, and pain with symptoms from specific categories. Since
ICC requires PEM/PENE and a sampling of other symptoms, it
may capture people with other complex chronic illnesses more easily than CCC.”
“I think that
CCC delimits the most homogeneous group.”
“The CCC is the best of the options
but open to criticism.”
“Fairly
comprehensive, and
clinician approved.”
“It has
the most required symptoms.”
“
CCC best fits many of the symptoms that the patients have, and it requires PEM. Any definition that doesn't require PEM shouldn't be used.”
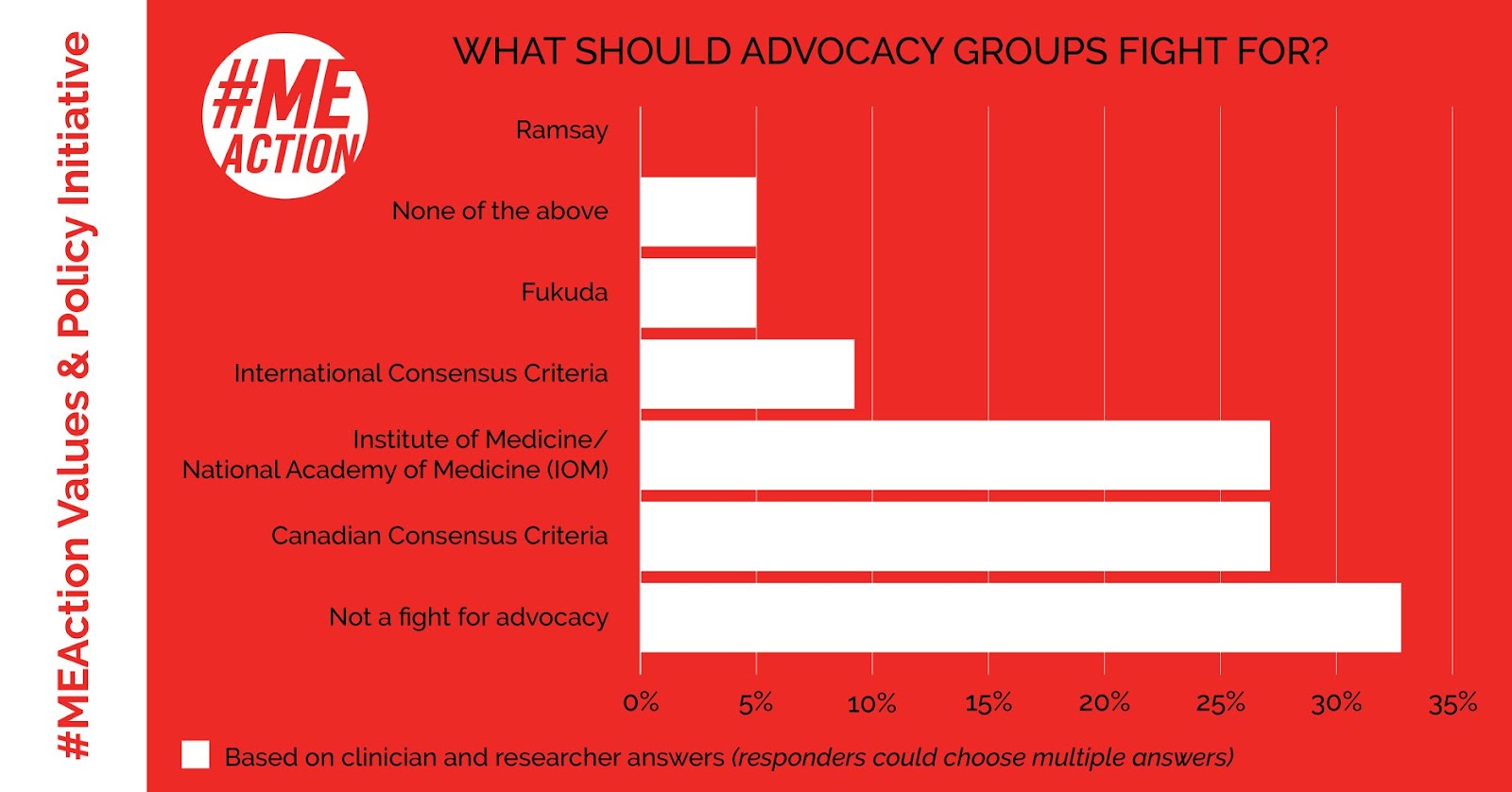
What should advocacy organizations fight for?
But is this what advocacy organizations should be working on?
The most common answer was no, with about 1/3 of responders in agreement.
About
1 out of 4 of ME-literate clinicians and researchers agreed advocating for the
Canadian Consensus Criteria was sensible, and the same number agreed on
NAM/IOM-related advocacy. Only two of the 22 responders agreed that ICC advocacy was a good choice.
One out of three researchers and clinicians don’t think advocacy organizations should fight for any particular set of criteria. Why not?
In their own words:
“The
support of the patient advocacy organizations has been fundamental for the advancements on ME/CFS research and health care.... However, I would
not single out any of them, as each of them have strong and weak points.”
“Tempted to say advocacy orgs should abandon advocating for any one set of criteria, but how we define the disease is important. It's more the snafu it creates with patients. My sense is that
the criteria have become more of a sense of identity for patients than anything related to research or clinical work, and that a lot of people are being
misled re: what constitutes evidence.”
“If patients’ organizations advocate for anything regarding definitions, I feel advocating for
more research comparing/ contrasting definitions is important. This doesn't mean just comparing symptom presentations but how
different definitions may lead to different prognoses, be
associated with different biomarkers/ etiologies, respond differently to treatment. Without good data, everything is speculation.
“Definitions in and of themselves aren't the end all: rather it's about how they can help clinicians care better for patients or help researchers learn more about a disease. My feeling is that
the lay public believes there is more evidence to inform which definition is the "best" than there currently is. Also, what the public believes to be good evidence is very different than what clinicians and researchers believe to be good evidence. Finally, patients can sometimes let emotion, popular opinion, etc, shape or sway their ideas too easily.
“Clinicians and scientists aren't immune to popularity or emotion either but the point is to be aware of and guard against such influences.
“
Early opposition in some circles against the NAM criteria may have set this whole field back, creating confusion, when current research continues to suggest that exertional intolerance is the heart of this illness. Some of that might be simply
a knee-jerk reaction to change rather than a careful assessment.”
Should we fight for one set of criteria? Which set of criteria, and if so, why?
")