Appalling, and so very foolish. Every single possible good news can't be taken for granted, everything can just be yanked away for no reason. I'm pretty sure there was a lot of lobbying from psychosomatic ideologues behind the scenes, there always is. Disgusting.Research and care funds are being reduced from around 150 million euros to just 16 million — a cut of nearly 90 percent. This happens despite studies estimating annual economic losses of over 63 billion euros, with total costs since the pandemic exceeding 250 billion euros.
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
News from Germany
- Thread starter TiredSam
- Start date
-
- Tags
- germany me/cfs news regional thread
Yann04
Senior Member (Voting Rights)
I can’t imagine what its like for the advocates who put their health on the line to campaign for this for so long. Just to have the government go “yeah nah”.Every single possible good news can't be taken for granted, everything can just be yanked away for no reason.
Chandelier
Senior Member (Voting Rights)

Long Covid - Der lange Schatten der Pandemie
Knapp sechs Jahre nach Beginn der Pandemie leiden viele Menschen unter den Langzeitfolgen einer Covid-19-Infektion. Axel Dorloff diskutiert am 11. November, um 17:30 Uhr in der Technologiestiftung Berlin mit seinen Gästen über aktuelle Forschungsergebnisse und Gesundheitsdaten sowie digitale...
 www.inforadio.de
www.inforadio.de
Upcoming Discussion: Long Covid – The Long Shadow of the Pandemic
Almost six years after the beginning of the pandemic, many people continue to suffer from the long-term effects of a Covid-19 infection. On November 11 at 5:30 p.m., Axel Dorloff will host a discussion at the Technologiestiftung Berlin with his guests about current research findings, health data, and digital infrastructures in the search for causes and effective therapies.
Panelists
Dr. Christian Gogoll, Specialist in Internal Medicine and Pulmonology, lead author of the Long Covid Patient Guideline
Max B. Eckert, Research Associate and Data Scientist at the CityLAB of the Technologiestiftung Berlin, co-developer of a post-Covid data model
Dr. Elisa Stein, Institute of Medical Immunology at Charité – Universitätsmedizin Berlin, researcher on Post-Covid and ME/CFS
Moderator: Axel Dorloff
Registration and Further Information
If you would like to attend, please register in advance via the following link:
https://www.technologiestiftung-berlin.de/veranstaltungen/long-covid-der-lange-schatten-der-pandemie
Venue: Technologiestiftung Berlin, Grunewaldstraße 61–62, 10825 Berlin
Date and Time: Tuesday, November 11, 2025, 5:30 p.m.
Chandelier
Senior Member (Voting Rights)
Handelsblatt
 www.handelsblatt.com
www.handelsblatt.com
AI Summary:
German Government Cuts Funding for Long Covid Research
The latest federal budget includes almost no new funding for Long Covid research, a decision that scientists criticize as short-sighted and potentially costly for the economy. Experts estimate that the long-term economic consequences could reach billions of euros.
Shrinking Budgets Despite Promises
In July, Health Minister Nina Warken (CDU) had expressed determination to support Long Covid research, promising substantial financial backing. However, the 2026 draft budget tells a different story. New research funding has been cut dramatically—from around €140–150 million in the previous legislative period under former Minister Karl Lauterbach (SPD) to only about €16 million.
Of this, €15 million is earmarked for care models for children and adolescents with Long Covid, and €200,000 for information and counseling services. Although Long and Post Covid are still listed as research priorities, the total health research budget of €41.47 million also covers seven other major areas, such as women’s health, digitalization, and prevention. These are not new funds but continuations of existing programs, and even this amount has been slightly reduced compared to last year (€43.08 million).
When asked about the lack of new funding, the Health Ministry referred vaguely to €118 million from ongoing programs but did not explain why no new money was allocated despite previous public promises.
Limited Support from the Research Ministry
The Federal Ministry of Education and Research (BMBF), led by Minister Dorothee Bär (CSU), is responsible for developing new treatments and medications. Although about €187 million is planned for “widespread diseases” in 2026—including cancer, heart disease, diabetes, dementia, and mental health—Long Covid is not listed separately. It is only indirectly supported through broader programs such as the National Network of University Medicine and ME/CFS research. Sources suggest that roughly €16 million of this total will benefit Long Covid projects.
Economic Costs and Health Consequences
According to the ME/CFS Research Foundation and partners, Long Covid and ME/CFS have already caused economic damages of over €250 billion in Germany since the pandemic began. Annual costs could reach €63 billion—about 1.5% of Germany’s GDP.
Economist Alexander Häring from the RWI-Leibniz Institute warns that cutting research will lead to higher long-term costs, as recovery often takes years and a lack of research slows the development of treatments and rehabilitation. Without government support, foundations and private institutions would have to fill the gap, though this is not a sustainable solution.
High Patient Numbers and Unmet Medical Needs
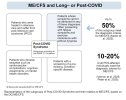
As of 2024, approximately 871,000 people in Germany were living with Long Covid and 650,000 with ME/CFS. Although some drugs have been approved for use, they were originally developed for other diseases. There is still no specific medication or therapy designed for Long Covid.
The need for research remains urgent, as each new infection increases the risk of developing the condition, and the social and psychological toll on patients continues to grow.
Wtf to those last three sections
Erkältung und Psyche: Fühlt sich an wie eine Depression, ist aber keine
Forschende entschlüsseln, was bei einer Erkältung mit der Psyche passiert. Woher das Leiden kommt und warum manche mehr jammern als andere.www.zeit.de
What a made up frankly product of a not right mind load of poisonous tosh. The sort of thing a really nasty person would use as Chinese whispers against some enemy and in a normal world most they’d try it with would take more from it about the teller and to watch out for them than the person it’s being said about
Bug the world seems to be going crazier atm
Chandelier
Senior Member (Voting Rights)

Anwalt verklagt Schulverwaltung: Berliner Schüler will in eine „Post-Covid-Klasse“
Wegen ihrer Long-Covid-Erkrankung fallen manche Kinder aus dem Schulsystem. Ein Anwalt erklärt im Interview, wieso er eine Spezialklasse für sie durchsetzen will.
 www.berliner-zeitung.de
www.berliner-zeitung.de
AI Summary:
Lawyer Sues Berlin School Authorities: Student Demands a “Post-Covid Class”
By Martin Rücker, October 23–24, 2025
Challenges for Students with Long Covid
For many children suffering from Long or Post Covid, regular school attendance is impossible. Some struggle only with physical activity, while others cannot tolerate classroom noise or sustain attention for several hours. The most severely affected are bedridden, and some experience alternating phases of illness and near-normal health. According to lawyer Friedrich Alexander Barthel, the Berlin school system often fails to provide the necessary flexibility for these children.
Lack of Understanding and Support
Barthel explains that many schools misunderstand the illness. Teachers sometimes doubt the legitimacy of absences when a child’s condition fluctuates, leading to a refusal to accept medical certificates. Children with Long Covid are legally entitled to home schooling under Berlin’s special education regulations—up to 16 hours per week. In practice, some receive only two hours or none at all. Barthel estimates that dozens of children who could be taught receive little or no instruction.
Legal Rights and Administrative Shortcomings
Schools often wrongly assume that home teaching depends on available staff. Barthel emphasizes that this right is unconditional. Even bedridden children can benefit from limited lessons. However, the total number of home teaching hours per district is capped at 100, forcing schools to divide the limited time among all sick students.
Proposal for “Post-Covid Classes”
To address isolation and lack of structure, Barthel is representing a family suing the Friedrichshain-Kreuzberg district and the Berlin education authority to establish a “Post-Covid class.” This special class would combine students from different grades who have Long Covid, allowing small groups of about five children to study together. Those unable to attend in person could join via digital avatars. Such classes would help maintain social contact and could even reduce teacher workload compared to one-on-one home lessons.
Resistance from Authorities
The district and the Berlin education administration oppose the idea, citing lack of space and logistical difficulties, since schools are organized by district rather than citywide. Barthel calls these arguments short-sighted, noting that many small unused rooms in old school buildings could serve such groups.
Use of Avatars as an Interim Solution
Some Berlin schools already use avatars—digital devices placed on a student’s desk that transmit lessons home and allow remote participation. Implementation, however, varies widely between districts. Barthel sees inconsistency in how school officials exercise their discretion in such cases.
Call for Political Action
Barthel urges the education senator to issue clear guidelines recognizing Long Covid as an organic disease. Without this classification, schools often treat affected children as psychologically ill, referring them to therapy rather than providing educational support or assistive tools like avatars. He also calls for clearer rules to ensure that schools and authorities act in the students’ best interests and for avatars to be legally recognized as educational aids.
Administrative and Technical Obstacles
Barthel criticizes communication barriers with schools, which are no longer reachable via fax and are not connected to the secure electronic legal communication system. Because emails are not legally binding, he must rely on postal mail, which is too slow and unreliable for urgent matters. This, he says, makes it difficult to represent students’ interests effectively and within legal time limits.
These four. I can take an informed guess at it, but would like to be certain. Thanks.What exactly would you like to have translated?
")




Chandelier
Senior Member (Voting Rights)
Slight overkillThese four. I can take an informed guess at it, but would like to be certain. Thanks.
 but I thought a picture recreation would be the least exhausting to comsume.
but I thought a picture recreation would be the least exhausting to comsume.Attachments


Chandelier
Senior Member (Voting Rights)

(S+) Long Covid: ME/CFS-Patientin über die psychischen Belastungen ihrer Krankheit
Ihre ME/CFS-Erkrankung reißt Natascha mit 29 Jahren aus dem Leben. Sie ist pflegebedürftig. Familie und Freundinnen kümmern sich um sie – und kämpfen mit ihr für eine bessere medizinische Versorgung.
Another big article about a very severe pwME in DER SPIEGEL.
Many patients experience that their illness is not taken seriously. Some even leave the hospital in worse condition than when they arrived. It was similar for Natascha.
“Not everything Taschi was afraid of happened—but almost everything,” Axel says calmly about the hospital stay. Together with Sophie and another friend, they attended the medical consultations. “We brought an entire folder with everything important,” he says. The attending neurologist was convinced that Natascha was psychotic and that ME/CFS was not a real disease.
In hospitals, activating patients is one of the main treatment goals. For ME/CFS patients, that’s poison, says Natascha’s general practitioner in the background interview. Sophie and Axel report that doctors and nurses ignored Natascha’s need for rest and her sensitivity to light. They tried to make her sit up—but with her level of illness, that was impossible. Her circulatory system collapsed.
At her own request, she was discharged after one week.
AI summary:
“When I Lie in the Dark, Rage Overcomes Me”
A Life Before the Darkness
Before her illness, Natascha S. was a lively young woman who loved music, dancing, and traveling. She studied in Göttingen, worked with young refugees in Leipzig, and was surrounded by a close circle of friends. At 29, her life changed abruptly when she developed ME/CFS (Myalgic Encephalomyelitis/Chronic Fatigue Syndrome). Now 31, she lives isolated in a darkened 15-square-meter room, entirely dependent on others for care.
Life in a Darkened Room
Natascha’s world is almost completely sealed off from light and sound. Her windows are taped shut, and anyone entering must wear an FFP2 mask and speak only in whispers. She cannot sit up, stand, or speak for long. Her daily existence revolves around pain management, rest, and survival. For the past 14 months, she has been bedridden. “I feel buried alive,” she whispers. She can no longer watch films, listen to music, or make phone calls. Every small act of independence—using a spoon, washing, communicating—is an exhausting effort.
The Invisible Disease
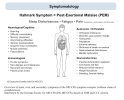
ME/CFS is a chronic, multisystem illness that can follow viral infections such as Epstein-Barr or Covid-19. It causes severe fatigue, pain, and hypersensitivity to stimuli. Germany has an estimated 650,000 patients, though many remain undiagnosed. Despite being classified by the WHO since 1969, ME/CFS is still poorly understood and under-researched. For those severely affected, even minimal exertion can cause a “crash”—a period of extreme worsening known as Post-Exertional Malaise. Natascha experiences these repeatedly.
Fighting Through the Pain
Because communication can trigger a crash, Natascha speaks in short whispers or via hand signals. To conduct interviews, she takes small doses of Tavor, a sedative that allows brief relief from pain. She cannot work, and her finances are strained; her family and friends support her through donations and care. “I’m trapped in my body,” she says quietly. Yet her will to live persists. Anger—at the system, at the neglect—is what keeps her alive.
Writing as Resistance
Unable to undergo therapy, Natascha turns to writing. On her Instagram account, she documents her illness and criticizes medical neglect and social discrimination. “When I lie in the dark, rage overcomes me,” she wrote once. Her activism has reached politicians, including former Health Minister Karl Lauterbach, who admitted systemic failures in ME/CFS care. For Natascha, writing is both emotional survival and political protest—an attempt to change the system from her bed.
Friendship and Survival
When her condition collapsed in 2024, friends Sophie and Axel became her full-time caregivers for three weeks. They fed, washed, and monitored her through sleepless nights, terrified she might die. Medical professionals often dismissed her condition as psychological. Their experience revealed the extent of institutional ignorance. Eventually, Natascha’s mother took over her care, and a small team of assistants now supports her daily needs. Each helper was chosen for understanding the political dimension of illness and disability.
Holding On to Small Joys
Despite constant pain, Natascha still finds fleeting beauty: the sound of rain, a bird’s call, the presence of a friend’s dog beside her bed. She dreams of having an assistance dog and, one day, enough strength to sit in a wheelchair again. Her friends describe her as astonishingly resilient, though the fear of losing her is constant. “I still have so much desire for life,” she whispers, even as she keeps the paperwork for assisted suicide near her bed—unfilled, but present.
Endurance in the Dark
Natascha’s story is one of isolation, friendship, and quiet defiance. She lives between exhaustion and anger, despair and hope. Her body confines her, but her words reach beyond the dark room. “How many more years can I endure this?” she asks. Yet she continues—alive, alert, and fighting for recognition, dignity, and the right to be seen.
Chandelier
Senior Member (Voting Rights)
Dysthymie : Die kleine Schwester der Depression
Es gibt Menschen, denen fehlt Freude und Energie im Leben. Wie bei einer Depression, nur anders. Dysthymie, sagen Experten. Der Übergang zur Krankheit ist fließend.
Fascinating how the article sets out to define dysthymia and ends up introducing a new diagnosis instead.
Dysthymia: The Little Sister of Depression
By Matthias Kreienbrink, November 2, 2025
What Dysthymia Feels Like
Some people live with a persistent lack of joy and energy—similar to depression, but not quite the same. This condition is called dysthymia, or dysthymic disorder. It involves a chronically low mood lasting at least two years, accompanied by symptoms such as low self-esteem, hopelessness, sleep or concentration problems. The symptoms resemble depression but are milder and do not meet the full criteria for a depressive episode.
Differences Between Dysthymia and Depression
According to psychiatrist Christian Otte from Charité Berlin, depression often appears suddenly with severe symptoms, while dysthymia is chronic and long-lasting. People with dysthymia often manage daily life but feel inner emptiness. Their hobbies or routines may remain intact, yet they bring little pleasure.
A Condition Once Seen as a Personality Trait
Psychiatrist Maximilian Deest notes that dysthymia was once called a “depressive personality disorder.” Patients often view it as part of who they are rather than an illness. It influences personality, interests, relationships, and self-worth. Unlike depression, it is experienced as a lifelong, stable state rather than a temporary episode.
Blurred Boundaries and Causes
The line between dysthymia and depression is fluid. Both can share roots in childhood trauma, neglect, or genetic and environmental factors. The disorders are better seen as part of a continuum rather than separate categories.
A Broader Diagnosis: Persistent Depressive Disorder
Modern classifications, such as the DSM-5, combine dysthymia and chronic depression into “persistent depressive disorder.” This captures both chronic low mood and recurring depressive episodes within one diagnosis.
Recognizing and Treating Dysthymia
Many affected individuals never seek help, believing their condition is normal. Therapy—especially CBASP, a form combining cognitive-behavioral and psychodynamic methods—is the primary treatment, sometimes supported by antidepressants. Structure, exercise, and social contact help recovery, though progress is often slow. As Deest emphasizes, chronic melancholy can be treated—it does not have to remain a lifelong state.
Chandelier
Senior Member (Voting Rights)

Miranda Wolpert: "In manchen Gruppen war das Achtsamkeitstraining sogar schädlich"
Miranda Wolpert erforschte jahrzehntelang, was psychische Probleme verhindert oder entschärft. Ihre Ergebnisse zeigen: Oft hilft nicht das, was wir glauben.
Miranda Wolpert spent decades researching what prevents or alleviates psychological problems. Her findings show that what actually helps is often not what we believe.
The Need for Scientific Rigor
Wolpert calls for the same scientific standards for psychosocial programs as for medications. Governments should implement interventions gradually and evaluate them systematically—like natural experiments. Well-meaning initiatives from NGOs and community groups are valuable, but passion alone is not enough.
AI Summary:
In Some Groups, Mindfulness Training Was Even Harmful
What Really Helps Mental Health
Miranda Wolpert, head of mental health research at the Wellcome Trust, has long studied what prevents or eases psychological problems in young people. Her research identifies around forty “active ingredients” across six categories that can promote mental well-being. These range from personal traits like openness and reduced perfectionism to environmental factors such as creative activities, a healthy microbiome, and strong neighborhood connections.
No Single Cure
Wolpert emphasizes that there is no universal solution for preventing mental illness. Many factors have only small effects, and what benefits one person at one time may not help another. In a large study comparing different school-based interventions—from yoga to behavioral therapy—no significant differences were found between methods. Wolpert suspects that the enthusiasm and commitment of teachers and facilitators might matter more than the specific techniques, though this has not been scientifically proven.
The Limits of Mindfulness
One striking finding concerns mindfulness programs in schools. A major Wellcome-funded study revealed that mindfulness training did not protect children under 13 from developing depression. In some groups, it was even harmful. Wolpert stresses that psychosocial interventions are often assumed to be harmless simply because they are well-intentioned, but this assumption is dangerous. Programs can fail—or even worsen emotional problems—if implemented without careful evaluation.
Why Some Interventions Fail
For adults, mindfulness-based stress reduction has strong evidence of effectiveness. For children, however, large-scale school programs often do not work. Wolpert suggests that students may not practice enough and that limited school time can make such training counterproductive. For example, mindfulness sessions can replace physical education, depriving children of activities that are proven to support mental health.
The Need for Scientific Rigor
Wolpert calls for the same scientific standards for psychosocial programs as for medications. Governments should implement interventions gradually and evaluate them systematically—like natural experiments. Well-meaning initiatives from NGOs and community groups are valuable, but passion alone is not enough. Effective mental health promotion requires both compassion and evidence.
Rethinking Mental Health in Youth
Wolpert challenges the idea that mental health divides neatly into “healthy” and “ill.” Research from New Zealand shows that 83 percent of people experience symptoms of a mental disorder at some point before age 35, but not continuously. Psychological distress often comes and goes. Many people recover without specialized treatment; about half of those who experience depression have only one episode in their lifetime.
The Role of Everyday Support
Wolpert argues that informal support—from teachers, peers, and social networks—plays a vital role. She urges educators not to fear mistakes but to engage with students’ emotional lives. Teachers, she says, can ask the same basic questions psychologists do: about friendships and life circumstances.
A Complex Picture of a Generation
While Wolpert acknowledges rising rates of depression and anxiety—especially among girls and young women—she also notes positive trends: declining substance abuse, risky behavior, and aggression. Despite the challenges, today’s youth are, in her words, “the most peaceful and least addicted generation ever.”
Sigh!!Miranda Wolpert: "In manchen Gruppen war das Achtsamkeitstraining sogar schädlich"
Miranda Wolpert erforschte jahrzehntelang, was psychische Probleme verhindert oder entschärft. Ihre Ergebnisse zeigen: Oft hilft nicht das, was wir glauben.
AI Summary:
Someone with common sense.
Yann04
Senior Member (Voting Rights)
Still not sure I’d fully trust them.Sigh!!
Someone with common sense.
Ie.
Her research identifies around forty “active ingredients” across six categories that can promote mental well-being. These range from personal traits like openness and reduced perfectionism to environmental factors such as creative activities, a healthy microbiome, and strong neighborhood connections.
But I do agree she seems far better than the average.
This would be a complete reset, as no psychosocial anything currently in use meets such standards. None. And very little psychological anything. This is exactly what's needed. Low standards only lead to one outcome: low standards.Wolpert calls for the same scientific standards for psychosocial programs as for medications.
Will that doctor be willing to accept conclusions that show no such thing? Because if there's one pattern that is unmistakable when it comes to such calls about reforms is that they are never about fixing the underlying problems, and are always, oh so coincidentally, perfectly tuned to elevate the caller-of-reform's pet ideology and beliefs. Always.For adults, mindfulness-based stress reduction has strong evidence of effectiveness.
It's more that most of the actually important skills are not taught and are hard to identify, especially to those who themselves don't have them. They're natural skills people either have or don't. We face something similar in the software industry, hiring good programmers is extremely difficult.Wolpert suspects that the enthusiasm and commitment of teachers and facilitators might matter more than the specific techniques, though this has not been scientifically proven.
Companies have spent fortunes trying to develop evaluation methods to the hiring process, only to find that most of the relevant skills are too hard to evaluate, even tend to be more among the 'soft' skills such as being able to work in teams or communicating ideas. Those methods don't work to identify such skills, and the only truly reliable way to assess the performance of a candidate is to employ them and have a good evaluation process as a continuing quality control measure.
There is no such evaluation process in health care. Once someone makes it through the certification, they are pretty much employed for life barring gross misconduct. The worst performers in health care are not weeded out, at worst they are shuffled around, sometimes to places where they have even less supervision and assessment, where they will do even more damage. Such as psychosomatics.
There has never been more mental health care and awareness than there has been in the last decade, despite many previously-asserted factors moving in the right direction. It's become frontline medicine, somehow, despite delivering absolutely nothing. In fact, it seems that the more is spent on mental health care and the more it creeps into medicine, the worse things are. Might be a coincidence. Might not be. No one can answer that question, which itself raises so many questions about what people are even doing here and why.While Wolpert acknowledges rising rates of depression and anxiety—especially among girls and young women—she also notes positive trends: declining substance abuse, risky behavior, and aggression. Despite the challenges, today’s youth are, in her words, “the most peaceful and least addicted generation ever.”
Chandelier
Senior Member (Voting Rights)

Forschungsgelder für ME/CFS: Versprechen gebrochen
Die Gesundheits- und die Forschungsministerin lasen Briefe von Betroffenen vor. Jetzt streicht die Regierung Forschungsgelder. Darauf noch ein Brief.
 taz.de
taz.de
AI translation:
Research Funding for ME/CFS Cut – Promises Broken
Commentary by Frederic Valin
On July 18, a video appeared on the official YouTube channel of the Federal Ministry of Health. In it, Health Minister Nina Warken and Research Minister Dorothee Bär read letters from people affected by ME/CFS (Editor’s note: Myalgic Encephalomyelitis/Chronic Fatigue Syndrome). They appeared visibly moved by the stories shared and promised to take action. Chancellor Friedrich Merz himself declared just two years ago: “Many sufferers rightly feel abandoned,” adding, “Every single ME/CFS case is one too many.”
Is that really so? The federal government has now decided to drastically cut ME/CFS research funding in the new budget. Promising therapeutic approaches already exist. One of the leading experts in the field, Prof. Dr. Carmen Scheibenbogen, has repeatedly stressed that her research could move forward immediately—if only studies were funded. For a year, she has been waiting for words to turn into action.
Let me remind you of your own statements. In July 2025, Minister Warken said that Germany bears “a special responsibility” in view of Long Covid and ME/CFS. You also expressed joy that both ministries were “in constructive exchange,” hoping to “set new impulses” and “raise the issue’s visibility through cooperation.”
In 2023, Chancellor Merz addressed the Bundestag, estimating 2.3 million people affected by Long Covid. He demanded that “for ten years, all forces in science, research, and practice” be united to ensure that “today’s tragedies become treatable diseases as quickly as possible.”
And now—silence. Not only are no new funds being approved, but existing ones are being cut. That is sheer cynicism. You know how much people suffer—yet you endorsed these austerity plans. You used their letters as emotional props for your social media presence. The few stories you read out hardly capture the daily realities of those living with ME/CFS.
It seems you never understood how essential the research you promised—and have now withdrawn—truly is. Funding was at least a signal that there was political will to help, to show people that they mattered.
More funding would not bring a cure overnight. But dedicating resources, refusing to forget, and striving to meet people’s needs and humanity—this was the least that could have been expected, and exactly what you so confidently promised.
Minister Warken, Minister Bär: you have done the opposite. You have instrumentalized these people to appear compassionate. After your strong words of support, you have instead put Level 1 care benefits up for debate, cut basic income support, and reduced research funding. And now, you remain silent.
Ministers Warken and Bär, who can still trust you and your coalition? Only those untouched by your decisions? Is that your idea of politics—of community?
Chandelier
Senior Member (Voting Rights)

Chronische Schmerzen : Man kann sich nicht an Schmerzen gewöhnen. Aber man kann sie verlernen
Hinter chronischem Schmerz verbirgt sich viel mehr als eine biologische Ursache. Wer die eigene Schmerzmatrix im Gehirn versteht, kann einen Weg hinaus finden.
You Cannot Get Used to Pain – But You Can Unlearn It
Behind chronic pain lies much more than a biological cause. Understanding one’s own pain matrix in the brain can open a way out.
A Long Struggle with Invisible Pain
For six years, 67-year-old Susanne Ganter has suffered from recurring nerve pain in her face. It began after a dental procedure, turning a mild discomfort into unbearable stinging. Despite numerous treatments—root canals, extractions, implants, massages, physiotherapy, and even osteopathy—nothing helped. Like many chronic pain patients, she searched desperately for a physical cause that no one could find. In Germany, nearly one in three people lives with chronic pain lasting longer than three months, often without clear answers.
When the Body Sounds a False Alarm
Acute pain serves as a vital warning signal, alerting us to injury or danger. Normally, it subsides once the cause is treated. But sometimes, the pain persists without purpose—like a smoke alarm that won’t stop ringing. The body cannot adapt to pain; instead, it remains under constant stress. Those affected often face frustration and helplessness when doctors fail to provide relief.
How the Pain Memory Forms
The persistence of pain is linked to how the nervous system processes signals. Repeated activation of pain fibers lowers their threshold, making them fire more easily. Over time, these pathways become reinforced—like a trail that turns into a wide road. This process forms a “pain memory,” where even slight stimuli cause severe pain. Chronic pain arises partly from this biological sensitization and partly from emotional and psychological factors such as stress, mood, or past experiences.
The Brain’s Pain Matrix
Pain perception involves several brain regions, collectively called the pain matrix. It includes areas responsible for emotion and memory, which compare new pain signals with past experiences. This explains why emotions like fear or trauma can intensify pain. Studies show that people with stronger emotional responses exhibit greater brain activity in these regions. Thus, chronic pain is not just physical—it is also shaped by how individuals interpret and emotionally process their suffering.
The Power of the Mind
Chronic pain often leads to depression, anxiety, and social withdrawal. Psychological distress can both result from and contribute to pain. Financial worries, repeated sick leaves, or fear of job loss may worsen symptoms. The economic burden in Germany is estimated at 38 billion euros annually. Because of this complex interplay, experts emphasize that biological, psychological, and social factors must be treated together.
Beyond Pills and Surgery
Many patients rely on medication, including opioids, but these are rarely effective for chronic pain in the long term. According to experts, drugs should only bridge the gap until other measures take effect. The most effective approach is the interdisciplinary multimodal pain therapy, which combines medical, psychological, and physical treatments. Yet many patients reach such centers only after years of ineffective interventions.
Learning to Live with Pain
At the University Hospital in Freiburg, Susanne Ganter joined a four-week multimodal program. Patients learn what chronic pain is, how it arises, and how to manage it. The goal is not to eliminate pain but to regain control over life. Through education, group therapy, and physiotherapy, patients develop tools to function and set personal goals. Pain can indeed be “unlearned,” though this requires time and persistence.
Movement and Mindfulness as Medicine
Physical activity is one of the most effective treatments for chronic pain. Exercise activates nerve pathways that suppress pain signals and positively influences brain regions regulating emotion. Patients also learn pacing—balancing activity and rest—and to overcome fear of movement. For Ganter, this extended beyond exercise: she practiced setting boundaries in her personal life, avoiding overexertion and stress.
A New Relationship with Pain
More than six months later, Ganter’s pain remains but feels less threatening. She now understands that her brain, not her body, signals danger. “I know I’m safe,” she says. The tooth is fine; the alarm is false. She has learned calmness—and that pain, once learned, can indeed be unlearned.
Chandelier
Senior Member (Voting Rights)
800 word article about a pwME in the Augsburger Allgemeine:

 www.augsburger-allgemeine.de
www.augsburger-allgemeine.de
AI Sunmary:
Leben mit Long Covid: Wie eine Augsburgerin um Anerkennung kämpft
Mehr als eine Million Menschen in Deutschland leiden unter Long Covid und ME/CFS. Betroffene erleben mangelnde medizinische Versorgung und kämpfen um Anerkennung. Die Politik reagiert nur langsam.
AI Sunmary:
Life with Long Covid: How a Woman from Augsburg Fights for Recognition
A Life Interrupted
Anna, a 34-year-old environmental engineer from Bavaria, once lived for nature, travel, and concerts. After contracting Covid-19 in 2022, everything changed. She developed ME/CFS, a severe neuroimmunological illness that has confined her mostly to bed. “My whole life has changed,” she says. “Sometimes I feel like I’m losing my personality.”
A Widespread but Overlooked Illness
Over 1.5 million people in Germany suffer from ME/CFS or Long Covid, with real numbers likely higher due to underdiagnosis. A 2024 study estimated the economic cost at 63.1 billion euros. Despite political promises of research and support, patients face a medical system lacking understanding and resources.
Living with ME/CFS
After her infection, Anna experienced extreme exhaustion and her first “crash”—a hallmark of the disease where minimal effort worsens symptoms. She now spends about 20 hours a day lying down, struggling with pain, heart palpitations, and cognitive problems.
Recognition and Research
Although ME/CFS has been recognized by the WHO since 1969, awareness grew only after Covid-19. The German government now funds 34 research projects with 118 million euros until 2028. Still, many doctors dismiss symptoms as psychological, leaving patients feeling invalidated.
A Fight for Dignity
Anna’s path to disability pension was exhausting, marked by skepticism from authorities. Supported by her family and partner, she continues to hope and connect with others facing the same struggle.
Honestly, this is just sadistic. "It doesn't work, but we got them to sign a form saying it worked", or whatever.More than six months later, Ganter’s pain remains but feels less threatening.
A lot of problems with humanity right now have to do with lack of shame. We would do so much better as a species if people doing shameful things would feel shame. I don't understand how people involved in this aren't ashamed of what they are doing. This is total pseudoscience, as delusional as any other faith-based system.
But instead they are rewarded. And on and on it loops.
Chandelier
Senior Member (Voting Rights)
Interestingly, the article refers to the official german guidelines: https://register.awmf.org/assets/guidelines/053-036l_S1_Chronischer_Schmerz_2025-02.pdfHonestly, this is just sadistic. "It doesn't work, but we got them to sign a form saying it worked", or whatever.