Colleen Steckel
Senior Member (Voting Rights)
Worth noting a few of the objections being voiced...
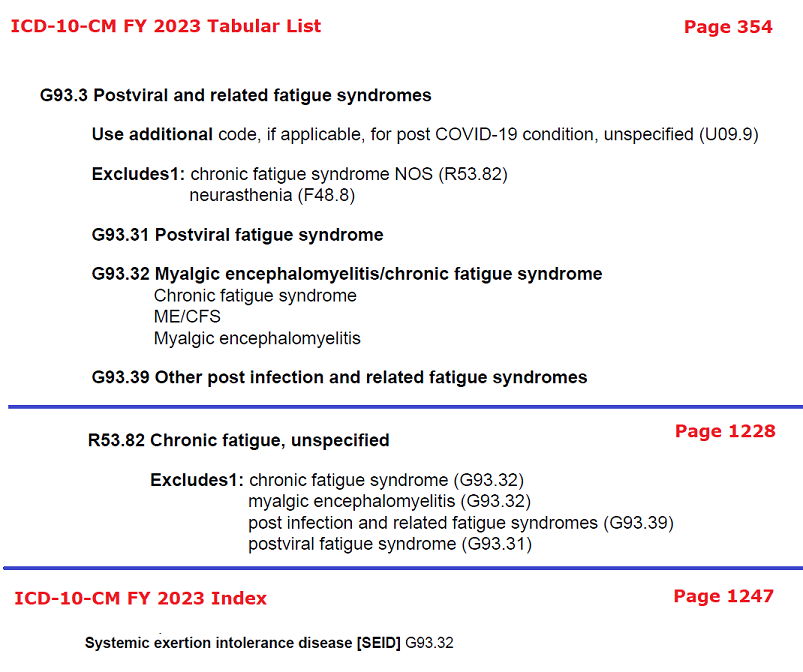
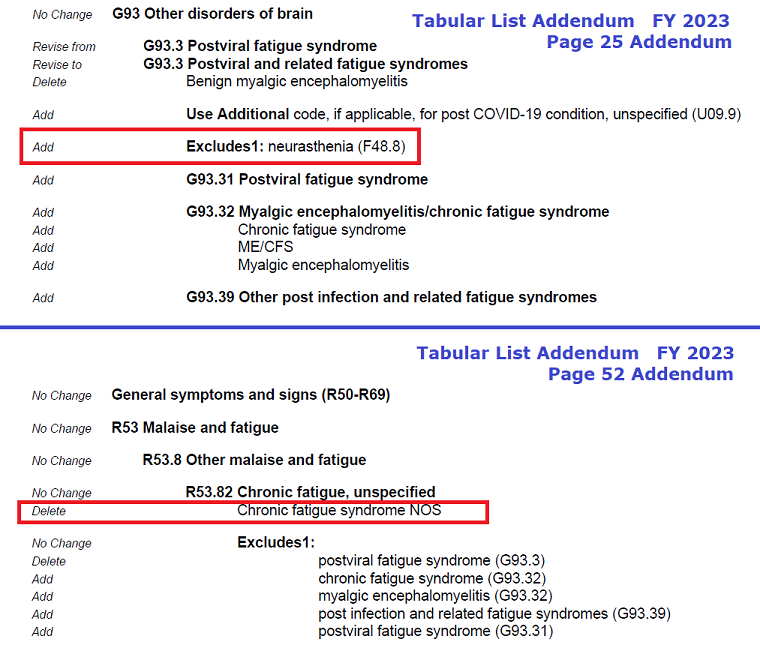
ME-International's proposal/comment calls for a) ME to only be diagnosed using the ME-ICC and b) the term CFS to be left in the symptoms chapter at R53.82 where it's equated to "chronic fatigue, unspecified." Then, if patients meet the IOM criteria or Canadian Consensus criteria but not the ME-ICC, it calls for them to be diagnosed with CFS and given the code R53.82. While the submission does not mention the 2021 NICE ME/CFS criteria, presumably the same logic would apply
This is from their submission (p. 7)
Those who fit the ME/CFS criteria as defined in either the Canadian Consensus Criteria or the IOM/NAM report (as shown on the CDC website) also need to be thoroughly screened using the ME IC Primer. If they fit the ME-ICC criteria they need to be given the ME diagnosis and the G93.3 label. If they do not have ME as per the ICC they would be given the CFS label and the R53.82 code.
This submission also rejects the addition of a code for the term ME/CFS.
So given the US uses the IOM criteria, this submission is calling for US patients diagnosed with ME/CFS to continue being dumped into and lost in the "chronic fatigue, unspecified" bucket unless the patient can convince the doctor to rediagnose them with the ME-ICC criteria instead and the patient meets the ME-ICC.
For its part, the Nightingale Research Foundation objects to this proposal in part because ME can only ever be triggered by an enterovirus. Lots of research countering that one.
[edited for clarity]
Please note the following clarifications
1. The part of the submission you refer to about those who fit the ME/CFS criteria need to be thoroughly screened is based on the expert guidance in the #MEICPrimer.
"Our panel strongly recommends that only the name ‘myalgic encephalomyelitis’ be used to identify patients meeting the ICC because a distinctive disease entity should have one name. Patients diagnosed using broader or other criteria for CFS or its hybrids (Oxford, Reeves, London, Fukuda, CCC, etc.) should be reassessed with the ICC. Those who fulfill the criteria have ME; those who do not would remain in the more encompassing CFS classification." pg ii.
As that was written in 2012 and the IOM report did not come out until 2015, the submission included the ME/CFS-IOM (SEID) criteria.
And, yes, ME International does support all patients get thorough screening to clarify what diagnosis is appropriate. The screening recommended includes the thorough biological testing on page 11 of the ME ICPrimer.
I do not think anyone who belongs in the ME Criteria would be left out by using the ME-ICC with the #MEIC Primer. The purpose of making sure everyone is thoroughly screened is to overcome the obstacle of doctors who don't understand ME.
2. The submission clarifies that the term ME/CFS as per the IOM is not referring to one patient group as it is an umbrella term that combined ME & CFS patient groups into one broad group. As stated above those who are in that broad group need to go on to be screened for ME.
3. This comment "US patients diagnosed with ME/CFS to continue being dumped into and lost in the "chronic fatigue, unspecified" bucket" couldn't be further from the truth.
I think we can all agree that no one should ever be dumped in the chronic fatigue unspecified bucket. The purpose for making sure ALL patients are thoroughly screened is to give them the best chance at getting personalized medicine and targeted treatments. Too often patients are sent home to modify their behavior by pacing/diet/salt intake with no other medical intervention offered. The ME IC Primer offers a LOT more in the way of testing and treatments. We want everyone to be given this level of care.
I believe the challenge comes down to a disagreement about the value of the IOM report as a diagnostic tool leading to a distinct disease. While some organizations/advocates feel the ME/CFS-IOM diagnosis is sufficient for all patients, there is a growing number of advocates, patients & researchers who feel this is inadequate for ME patient care and research and are advocating for acceptance worldwide of the ICC. The experts explain this much better than I can.
"The rationale for the development of the ICC was to utilize current research knowledge to identify objective, measurable and reproducible abnormalities that directly reflect the interactive, regulatory components of the underlying pathophysiology of ME. Specifically, the ICC select patients who exhibit explicit multi-systemic neuropathology, and have a pathological low threshold of physical and mental fatigability in response to exertion. Cardiopulmonary exercise testretest studies have confirmed many post-exertional abnormalities. Criterial symptoms are compulsory and identify patients who have greater physical, cognitive and functional impairments. The ICC advance the successful strategy of the Canadian Consensus Criteria (CCC) of grouping coordinated patterns of symptom clusters that identify areas of pathology. The criteria are designed for both clinical and research settings."
For those who may not be aware of who all was involved in writing the ME IC Primer - they are some of the most well known respected clinicians and researchers in our field.
From pg ii: An International Consensus Panel, consisting of clinicians, research investigators, teaching faculty, and an independent educator, represent diverse backgrounds, medical specialities and geographical regions. Collectively, the members of the panel have: • diagnosed and/or treated more than 50 000 patients who have ME; • more than 500 years of clinical experience; • approximately 500 years of teaching experience; • authored hundreds of peer-reviewed publications, as well as written chapters and medical books; and • several members have co-authored previous criteria.
Primer: https://www.me-international.org/uploads/1/2/7/6/127602984/me_icprimer_2015.pdf