Dx Revision Watch
Senior Member (Voting Rights)
Preparing for implementation of ICD-11 in NHS England:
https://digital.nhs.uk/about-nhs-di...preparations-for-the-implementation-of-icd-11
NHS Digital News
For information: Preparations for the implementation of ICD-11
26 January 2023:
Find out how to prepare for the next revision of the International Classifications of Diseases (ICD), ICD-11.
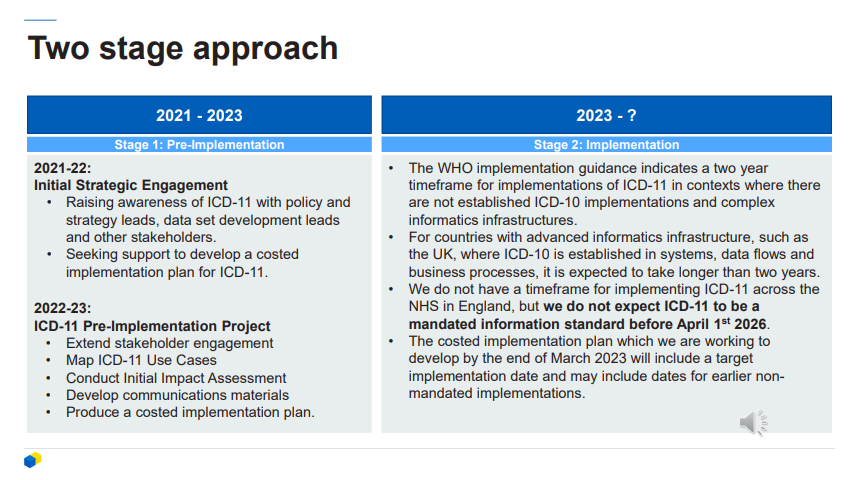
The next revision of the International Classifications of Diseases (ICD), ICD-11, is now approved by the WHO and will be mandated for use in the future. Our assumption is that ICD-11 will not be mandated for use across the NHS in England before April 2026, but to prepare for the changes, we are currently running an ICD-11 pre-implementation project to create a high-level implementation plan, which we aim to have ready in April 2023.
Find out more about our preparations for implementing ICD-11, as well as useful resources such as e-learning modules, ICD-11 API and coding tools, use cases and more. New content is being added continuously and we will also be scheduling interactive sessions with stakeholder groups over the coming months.
---------------------
More information on NHS England's preparation for adoption of ICD-11 here: https://nhsengland.kahootz.com/t_c_home/view?objectID=36254864
ICD-11 Pre-implementation overview presentation: https://nhsengland.kahootz.com/gf2..../PDF/-/ICD-11 Pre-Implementation Overview.pdf
https://digital.nhs.uk/about-nhs-di...preparations-for-the-implementation-of-icd-11
NHS Digital News
For information: Preparations for the implementation of ICD-11
26 January 2023:
Find out how to prepare for the next revision of the International Classifications of Diseases (ICD), ICD-11.
The next revision of the International Classifications of Diseases (ICD), ICD-11, is now approved by the WHO and will be mandated for use in the future. Our assumption is that ICD-11 will not be mandated for use across the NHS in England before April 2026, but to prepare for the changes, we are currently running an ICD-11 pre-implementation project to create a high-level implementation plan, which we aim to have ready in April 2023.
Find out more about our preparations for implementing ICD-11, as well as useful resources such as e-learning modules, ICD-11 API and coding tools, use cases and more. New content is being added continuously and we will also be scheduling interactive sessions with stakeholder groups over the coming months.
---------------------
More information on NHS England's preparation for adoption of ICD-11 here: https://nhsengland.kahootz.com/t_c_home/view?objectID=36254864
ICD-11 Pre-implementation overview presentation: https://nhsengland.kahootz.com/gf2..../PDF/-/ICD-11 Pre-Implementation Overview.pdf