hotblack
Senior Member (Voting Rights)
I’ve been thinking and reading more about dopamine. Partially because of interest in PD but also now in relation to eccentric medium spiny neurons aka eccentric spiny projection neurons (which have both D1 and D2 receptors).
I thought it would be useful to build up a list of dopamine modifying agents, how they modify things and look back at studies which have used them, perhaps with a different perspective or to be able to gain more of an understanding of potential mechanisms.
I’ll start of with some posts but please anyone jump in.
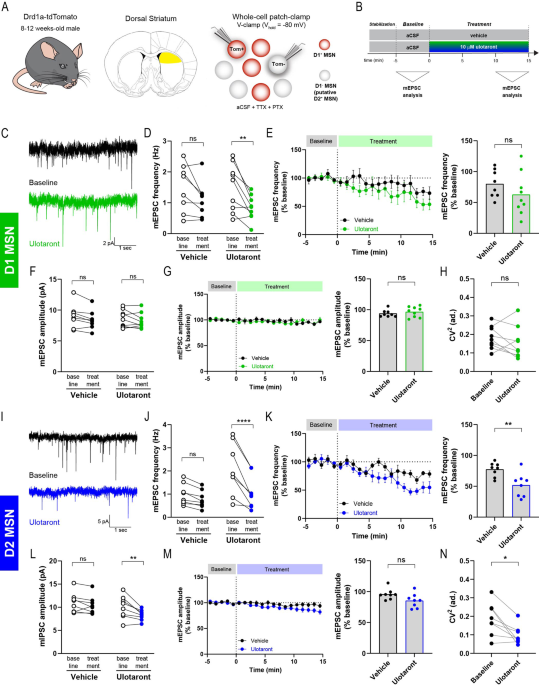
And from what I’ve read D1 generally excites the post-synaptic neuron while D2 generally dampens firing.
The most studied dopamine signaling pathway is the modulation of cyclic AMP production, with D1-like receptors activating cyclic AMP production through Gs/olf, and D2-like receptors inhibiting adenylyl cyclase (AC) activity through Gi/o proteins.
I thought it would be useful to build up a list of dopamine modifying agents, how they modify things and look back at studies which have used them, perhaps with a different perspective or to be able to gain more of an understanding of potential mechanisms.
I’ll start of with some posts but please anyone jump in.

") It’s probably going to be complicated enough so am trying to stick to more clearly understood dopamine modifiers.
It’s probably going to be complicated enough so am trying to stick to more clearly understood dopamine modifiers.