Do viruses cause permanent damage to receptors, though?Is it possible that glutamate synapses showing up in your results could be the result of Sars-cov-2 affecting mGlur2?
The details of GPCR–iGlu receptor cross-talk should inform a better understanding of how synaptic transmission is regulated and lead to new therapeutic strategies for neuropsychiatric disorders.
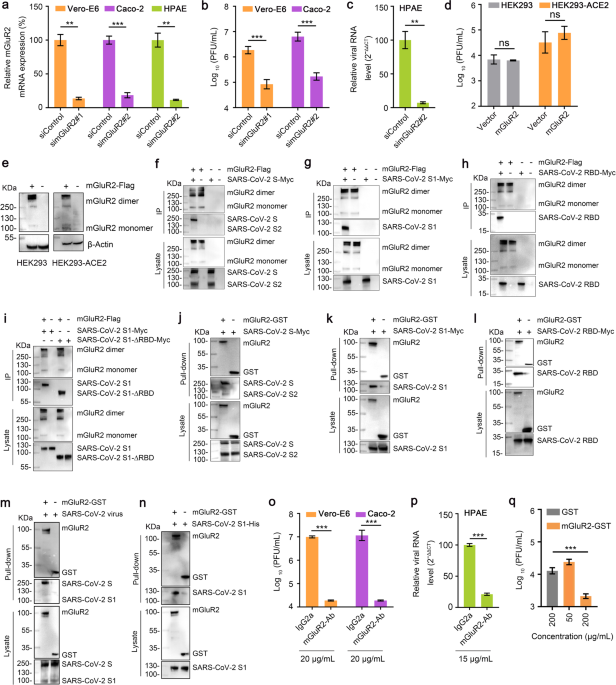
SARS-CoV-2 uses metabotropic glutamate receptor subtype 2 as an internalization factor to infect cells - Cell Discovery
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) uses angiotensin-converting enzyme 2 (ACE2) as a binding receptor to enter cells via clathrin-mediated endocytosis (CME). However, receptors involved in other steps of SARS-CoV-2 infection remain largely unknown. Here, we found that...www.nature.com
I can't find the answer.
"Virus–receptor interactions play a key regulatory role in viral host range, tissue tropism, and viral pathogenesis. Viruses utilize elegant strategies to attach to one or multiple receptors, overcome the plasma membrane barrier, enter, and access the necessary host cell machinery.
The viral attachment protein can be viewed as the “key” that unlocks host cells by interacting with the “lock”—the receptor—on the cell surface, and these lock-and-key interactions are critical for viruses to successfully invade host cells.
Many common themes have emerged in virus–receptor utilization within and across virus families demonstrating that viruses often target particular classes of molecules in order to mediate these events.
Common viral receptors include sialylated glycans, cell adhesion molecules such as immunoglobulin superfamily members and integrins, and phosphatidylserine receptors."
Something about viral entry, at least by enveloped viruses:
"Enveloped viruses can directly bind to and bypass the lipid bilayer of a host cell. Viral membrane fusion proteins (fusogens) facilitate this process by lowering the kinetic barrier of the bilayer – the fusogens bind to the host cell bilayer, undergo a conformational change and fuse the two bi-layers together."
This study maps the morphological changes in the plasma membranes of macrophages infected by human cytomegalovirus or human immunodeficiency virus and find novel differentially expressed receptors.
Viruses disregulate cell membrane receptors to become immune fugitives - Communications Biology
In order to maintain persistent infections, microbes that cause chronic disease have to evade detection by the human immune system. To do so, many modulate the expression of plasma membrane receptors that trigger cell signalling pathways and immune responses. Using microscopy and cell sorting...
www.nature.com