- Home
- Forums
- Guidelines, reviews and disease coding
- ME/CFS related guidelines, reviews, disease coding
- Disease coding
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
Updates on status of ICD-11 and changes to other classification and terminology systems
- Thread starter Dx Revision Watch
- Start date
Dx Revision Watch
Senior Member (Voting Rights)
Hopefully the US's ICD-10-CM, Canada's ICD-10-CA and other member states which use a national adaptation (aka "clinical modification") of ICD-10 will absorb this change to ICD terminology in future releases of their national adaptations.
InfiniteRubix
Senior Member (Voting Rights)
Profuse thanks, as always!
Dx Revision Watch
Senior Member (Voting Rights)
Profuse thanks, as always!
Thank you, InfiniteRubix.
The ICD-11 Orange Maintenance Browser implemented approval of this terminology change back in November 2020 - a decision which unfortunately came too late to be incorporated into the September 2020 update of the "Blue Browser". But it's good to see this ratified for the Blue Browser's May 2021 update, which was released this week.
Last edited:
Dx Revision Watch
Senior Member (Voting Rights)
Emerging briefly from retirement to update on the imminent completion of ICPC-3:
The International Classification of Primary Care, Second Edition (ICPC-2) is a WHO approved classification system that provides an international standard for systematically capturing and organising clinical information in primary care. It can be used to record reasons for encounter, practitioner's assessment of diagnosis, interventions and care plan. It has been the most widely used international classification system for ordering clinical data in primary care/general practice.
ICPC-2 is developed and maintained by WONCA (World Organization of National Colleges, Academies and Academic Associations of General Practitioners/Family Physicians aka the World Organization of Family Doctors).
The WHO has accepted ICPC-2 within the WHO-FIC [WHO Family of International Classifications] and there is a cross map between ICPC-2 and ICD-10 codes.
ICPC-2 is available in around 34 countries; is used in primary care in around 27 countries and is mandatory for use in primary care in 6 EU countries, which includes the Netherlands. Some countries, for example Denmark, have developed country specific extensions for which additional terms and sub codes have been inserted.
It has been translated into more than 20 languages.
Note that ICPC-2 is not mandated for use in NHS England which used the now retired Read Codes classification system. Since April 2018, the mandatory system for use in NHS England primary care has been SNOMED CT UK Edition.
The full ICPC-2 product is available on license but a two page PDF of summary codes is in the public domain: PDF ICPC-2 code list
Development of ICPC-3:
Since 2017, I have been mentioning in this thread and elsewhere that ICPC-2 has been under revision for ICPC-3. In September 2020, an invitation was issued for clinical professionals to register to field test the draft ICPC-3 but the revised codes and Description texts had not thus far been made available for public scrutiny and feedback.
I have also mentioned that back in 2010, the ICPC-2 maintenance and revision committee, which includes Dr Michael Klinkman (US GP) and Dr Marianne Rosendal (Project Manager and senior researcher, Functional Disorders, Aarhus University Hospital) had been discussing the potential for adding a Per Fink "Bodily distress syndrome (BDS)" type disorder construct to ICPC-3.
The ICPC-3 Project started in January 2018 and was expected to run for a period of three and half years. It has been developed by the ICPC-3 Consortium and the WONCA International Classification Committee (WICC).
According to the new ICPC-3 website, ICPC-3 will be published in paper format and as an eBook. Both versions "will be less detailed than the electronic format, but will contain a manual on how to use the ICPC-3 and a representative part of the ICPC-3 Classification for daily desk use."
It appears that the project is approaching completion although the print version of the book and manual and the eBook are still being edited.
It is not possible to estimate how long it will take for countries currently using ICPC-2 to adopt and migrate to ICPC-3 or how long it will take to develop national extensions and prepare translations.
A publicly accessible ICPC-3 Browser is already available where codes and disorder descriptions can be viewed without the need for registering for access. Comments can be uploaded subject to a brief registration process. Proposals for annual updates to the ICPC-3 can also be submitted following registration.
The ICPC-3 website from which the browser can be accessed can be found here: https://www.icpc-3.info
According to the project's Information Sheets:
"...A new version ICPC-3 has been adopted by WONCA in December 2020 and endorsed on April 16, 2021 during the WONCA Executive meeting."
"...The content of ICPC-3 remains closely 'linked' to relevant related international classifications, including ICD-10, ICD-11, ICF, ICHI, clinical terminologies such as SNOMED CT, and also to previous versions of ICPC-1, ICPC-2.7 and to the goals of WHO, such as Universal Health Coverage (UHC) and the Global Burden of Disease (GBD)."
"...ICPC is formally recognised by the World Health Organization's (WHO) Family of International Classifications (WHO-FIC) as a classification for primary care. The new ICPC-3 is already used by the WHO - Primary Health Care department in the context of the Universal Health Care (UHC) Compendium as a structuring Framework and is linked to the WHO International Classifications. This allows communication between the ICPC-3 and the other classifications and complementary usage. Ongoing cooperation between WONCA and the WHO PHC and WHO-FIC network exists for the harmonization of the ICPC-3 with the UHC Compendium and the classifications of WHO, ICD-10, ICD-11, ICF and ICHI."
Note that I am retired now and I am not intending to submit comments or proposals for improvements.
If advocates or patient groups want to submit a proposal to improve the ICPC-3 classification or submit a comment on existing content you can do so in the ICPC-3 Browser. If you don't have an account you can register by clicking Register in the upper right corner of the ICPC-3 Browser.
"How to submit a proposal
After registration you can submit and view update proposals.
How does the Update Platform work?
Instructions:
All fully completed proposal will be reviewed by a team consisting of Medical Content Experts and Classification Experts and processed further in a number of steps.
The final date for update proposals is by the first of June of each year. If the update proposal was accepted it will become effective as of the first of January of the following year.
If you have an account then login and browse to the code for which you want to submit a proposal. After selecting the relevant code, enter your proposal in the lower left window and press Add Proposal. Please make sure to include a reference to the relevant literature supporting your proposal. Alternatively, you may mail the relevant documentation to info@icpc-3.info."
Continued in next post
Edited for clarity
The International Classification of Primary Care, Second Edition (ICPC-2) is a WHO approved classification system that provides an international standard for systematically capturing and organising clinical information in primary care. It can be used to record reasons for encounter, practitioner's assessment of diagnosis, interventions and care plan. It has been the most widely used international classification system for ordering clinical data in primary care/general practice.
ICPC-2 is developed and maintained by WONCA (World Organization of National Colleges, Academies and Academic Associations of General Practitioners/Family Physicians aka the World Organization of Family Doctors).
The WHO has accepted ICPC-2 within the WHO-FIC [WHO Family of International Classifications] and there is a cross map between ICPC-2 and ICD-10 codes.
ICPC-2 is available in around 34 countries; is used in primary care in around 27 countries and is mandatory for use in primary care in 6 EU countries, which includes the Netherlands. Some countries, for example Denmark, have developed country specific extensions for which additional terms and sub codes have been inserted.
It has been translated into more than 20 languages.
Note that ICPC-2 is not mandated for use in NHS England which used the now retired Read Codes classification system. Since April 2018, the mandatory system for use in NHS England primary care has been SNOMED CT UK Edition.
The full ICPC-2 product is available on license but a two page PDF of summary codes is in the public domain: PDF ICPC-2 code list
Development of ICPC-3:
Since 2017, I have been mentioning in this thread and elsewhere that ICPC-2 has been under revision for ICPC-3. In September 2020, an invitation was issued for clinical professionals to register to field test the draft ICPC-3 but the revised codes and Description texts had not thus far been made available for public scrutiny and feedback.
I have also mentioned that back in 2010, the ICPC-2 maintenance and revision committee, which includes Dr Michael Klinkman (US GP) and Dr Marianne Rosendal (Project Manager and senior researcher, Functional Disorders, Aarhus University Hospital) had been discussing the potential for adding a Per Fink "Bodily distress syndrome (BDS)" type disorder construct to ICPC-3.
The ICPC-3 Project started in January 2018 and was expected to run for a period of three and half years. It has been developed by the ICPC-3 Consortium and the WONCA International Classification Committee (WICC).
According to the new ICPC-3 website, ICPC-3 will be published in paper format and as an eBook. Both versions "will be less detailed than the electronic format, but will contain a manual on how to use the ICPC-3 and a representative part of the ICPC-3 Classification for daily desk use."
It appears that the project is approaching completion although the print version of the book and manual and the eBook are still being edited.
It is not possible to estimate how long it will take for countries currently using ICPC-2 to adopt and migrate to ICPC-3 or how long it will take to develop national extensions and prepare translations.
A publicly accessible ICPC-3 Browser is already available where codes and disorder descriptions can be viewed without the need for registering for access. Comments can be uploaded subject to a brief registration process. Proposals for annual updates to the ICPC-3 can also be submitted following registration.
The ICPC-3 website from which the browser can be accessed can be found here: https://www.icpc-3.info
According to the project's Information Sheets:
"...A new version ICPC-3 has been adopted by WONCA in December 2020 and endorsed on April 16, 2021 during the WONCA Executive meeting."
"...The content of ICPC-3 remains closely 'linked' to relevant related international classifications, including ICD-10, ICD-11, ICF, ICHI, clinical terminologies such as SNOMED CT, and also to previous versions of ICPC-1, ICPC-2.7 and to the goals of WHO, such as Universal Health Coverage (UHC) and the Global Burden of Disease (GBD)."
"...ICPC is formally recognised by the World Health Organization's (WHO) Family of International Classifications (WHO-FIC) as a classification for primary care. The new ICPC-3 is already used by the WHO - Primary Health Care department in the context of the Universal Health Care (UHC) Compendium as a structuring Framework and is linked to the WHO International Classifications. This allows communication between the ICPC-3 and the other classifications and complementary usage. Ongoing cooperation between WONCA and the WHO PHC and WHO-FIC network exists for the harmonization of the ICPC-3 with the UHC Compendium and the classifications of WHO, ICD-10, ICD-11, ICF and ICHI."
Note that I am retired now and I am not intending to submit comments or proposals for improvements.
If advocates or patient groups want to submit a proposal to improve the ICPC-3 classification or submit a comment on existing content you can do so in the ICPC-3 Browser. If you don't have an account you can register by clicking Register in the upper right corner of the ICPC-3 Browser.
"How to submit a proposal
After registration you can submit and view update proposals.
How does the Update Platform work?
Instructions:
- Select a four digit (AA00) class for which you would like to make an update proposal.
- Select a specific type of proposal in the dropdown menu:
- Proposal to improve the text of the preferred rubric
- Proposal to improve the text of the description rubric
- Proposal to improve, add or remove an inclusion rubric
- Proposal to Improve, add or remove a reference to an external classification
- Proposal to add a new category (ie code with 4 digits)
- Proposal to add a new regional category (ie code with 6 digits) - Explain in the empty text box under Proposal what your suggestion is, and indicate the exact code, class-name and Id if available.
- After the selection you need to select the type of motivation from the dropdown menu and describe in detail what the motivation is for the proposal. You also need to include a reference to support your update proposal. Without a reference your update proposal cannot be processed.
- Consider if your proposal has any consequences for other classes in the ICPC-3 and if this is the case, indicate which code(s) is affected.
All fully completed proposal will be reviewed by a team consisting of Medical Content Experts and Classification Experts and processed further in a number of steps.
The final date for update proposals is by the first of June of each year. If the update proposal was accepted it will become effective as of the first of January of the following year.
If you have an account then login and browse to the code for which you want to submit a proposal. After selecting the relevant code, enter your proposal in the lower left window and press Add Proposal. Please make sure to include a reference to the relevant literature supporting your proposal. Alternatively, you may mail the relevant documentation to info@icpc-3.info."
Continued in next post
Edited for clarity
Last edited:
Dx Revision Watch
Senior Member (Voting Rights)
Continued from previous post
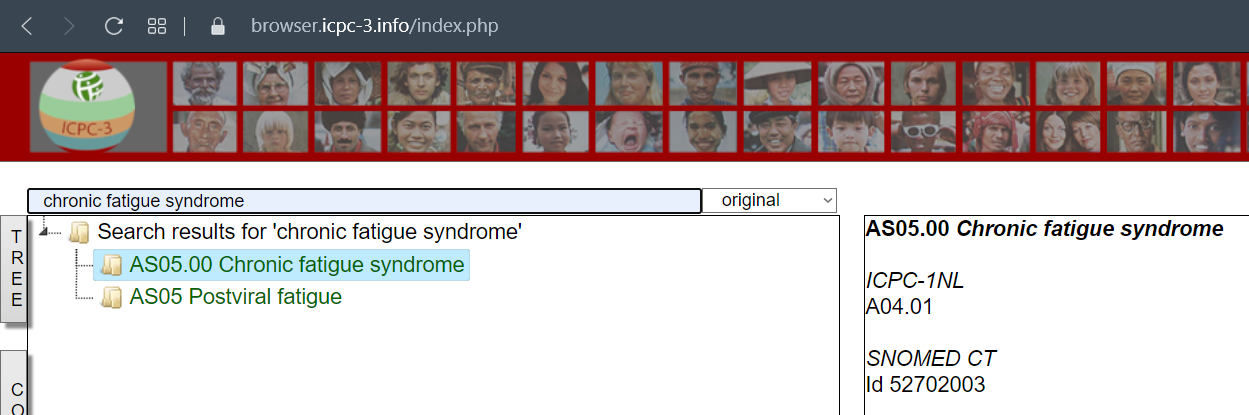
ICPC-3 Browser:
https://browser.icpc-3.info/index.php
Registration is required in order to submit comments or proposals.
Note there is a Search box at the top of the code tree:
There are conversion tables here for ICPC-3 to ICPC-2 to ICPC-1:
Conversion tables
https://www.icpc-3.info/documents/extra/conversion-table-icpc-3.pdf
This is the listing for Chronic fatigue syndrome and Postviral fatigue [sic] in ICPC-3 (my notes in blue and in brackets):
(In ICPC-2, Chronic fatigue syndrome used the A04 Weakness/tiredness general code.
For ICPC-3, there are two new codes: AS05 Postviral fatigue and its Inclusion AS05.00 Chronic fatigue syndrome which are listed under the "General" A codes. Myalgic encephalomyelitis is listed as an Index term to AS05. These terms are cross mapped to ICD-10 G93.3 and ICD-11 8E49.
There is an Exclusion under these two codes for ICPC-3's AS04 weakness/tiredness, general code.
The Descriptive text is execrable and needs comments and proposals for revision submitting by advocates, patient groups, clinical allies etc.)
Section A General
AS General symptoms, complaints and abnormal findings
AS05 Postviral fatigue
AS05.00 Chronic fatigue syndrome
AS05 Postviral fatigue
Description
Postviral fatigue is characterised by persistent or recurrent fatigue, diffuse musculoskeletal pain, sleep disturbances, and subjective cognitive impairment of 6 months duration or longer. Symptoms are not caused by ongoing exertion; are not relieved by rest; and result in a substantial reduction of previous levels of occupational, educational, social or personal activities. Minor alterations of immune, neuroendocrine, and autonomic function may be associated with postviral fatigue.
Chronic fatigue syndrome: considerable cultural variations occur in the presentation of this problem, and two main types occur, with substantial overlap. In one type, the main feature is a complaint of increased fatigue after mental effort, often associated with some decrease in occupational performance or coping efficiency in daily tasks. The mental fatiguability is typically described as an unpleasant intrusion of distracting associations or recollections, difficulty in concentrating, and generally inefficient thinking. In the other type, the emphasis is on feelings of bodily or physical weakness and exhaustion after only minimal effort, accompanied by a feeling of muscular aches and pains and inability to relax. In both types a variety of other unpleasant physical feelings is common, such as dizziness, tension headaches, and feelings of general instability. Worry about decreasing mental and bodily well-being, irritability, anhedonia, and varying minor degrees of both depression and anxiety are all common. Sleep is often disturbed in its initial and middle phases but hypersomnia may also be prominent.
Inclusion
chronic fatigue syndrome AS05.00
Exclusion
weakness/tiredness, general AS04
Index terms
chronic fatigue syndrome
myalgic encephalomyelitis
ICPC-1
A04
ICPC-2
A04
ICD10
Postviral fatigue syndrome G93.3
ICD11
Postviral fatigue syndrome 8E49
SNOMED CT
chronic fatigue syndrome = myalgic encephalomyelitis Id 52702003
postviral fatigue syndrome (disorder) Id 51771007
-------------------------------------------
This is the listing for "Bodily distress or somatisation disorder" in ICPC-3 (my comments in blue and in brackets):
Section P Psychological, mental and neurodevelopmental
PD Psychological, mental and neurodevelopmental diagnoses and diseases
PD10 Bodily distress or somatisation disorder
(New code PD10 Bodily distress or somatisation disorder replaces ICPC-2 code P75 Somatisation disorder.)
Description
Bodily distress disorder is characterised by the presence of bodily symptoms that are distressing to the individual and excessive attention directed toward the symptoms, which may be manifest by repeated contact with health care providers. If another health condition is causing or contributing to the symptoms, the degree of attention is clearly excessive in relation to its nature and progression. Excessive attention is not alleviated by appropriate clinical examination and investigations and appropriate reassurance. Bodily symptoms are persistent, being present on most days for at least several months. Typically, bodily distress disorder involves multiple bodily symptoms that may vary over time. Occasionally there is a single symptom, usually pain or fatigue, that is associated with the other features of the disorder.
(This Description text is identical to ICD-11's Description text for "Bodily distress disorder" apart from omission of the final sentence of ICD-11's BDD Description text, which reads:
"...The symptoms and associated distress and preoccupation have at least some impact on the individual’s functioning (e.g. strain in relationships, less effective academic or occupational functioning, abandonment of specific leisure activities)."
Inclusion
somatization disorder
Index terms
bodily distress disorder
conversion disorder (This term does not align with ICD-11 which classifies "Dissociative neurological symptom disorder" - the ICD-11 equivalent of "conversion disorder" - under Dissociative disorders, not under BDD.)
pseudocyesis (This term is coded to F45.8 in ICD-10. "Pseudocyesis" [phantom pregnancy] is not included in ICD-11, as far as I can determine.)
somatic symptom [sic] (I think this should read "somatic symptom disorder" if they intend to align with ICD-11's list of Synonyms terms under BBD.)
somatoform disorder
(They have omitted ICD-11's list of exclusion terms, which includes excludes for PVFS, ME; and CFS under BDD.)
ICPC-1
P75
ICPC-2
P75
ICD10
no exact coresponding [sic] class 00
Somatization disorder F45.0
Undifferentiated somatoform disorder F45.1
ICD11
Bodily distress disorder 6C20
SNOMED CT
bodily distress disorder Id 723916001
somatization disorder Id 397923000
somatoform disorder Id 31297008
------------------------------------
It appears that the developers of ICPC-3 have chosen to revise ICPC-2's P75 term to align with ICD-11's Bodily distress disorder construct and have not included Fink's BDS term and disorder construct within the revised classification, as far as I can see; they are cross mapping code PD10 Bodily distress or somatisation disorder to ICD-11's 6C20 Bodily distress disorder, and to SNOMED CT's 723916001 Bodily distress disorder.
As I say, I am not intending to comment on the content of ICPC-3 or submit proposals for improvements since I am retired, but I would urge advocates and patient groups to submit for improvements, particularly in those countries which currently use ICPC-2 in primary care (Denmark, Netherlands and others).
Edited for clarity and to insert image
ICPC-3 Browser:
https://browser.icpc-3.info/index.php
Registration is required in order to submit comments or proposals.
Note there is a Search box at the top of the code tree:
There are conversion tables here for ICPC-3 to ICPC-2 to ICPC-1:
Conversion tables
https://www.icpc-3.info/documents/extra/conversion-table-icpc-3.pdf
This is the listing for Chronic fatigue syndrome and Postviral fatigue [sic] in ICPC-3 (my notes in blue and in brackets):
(In ICPC-2, Chronic fatigue syndrome used the A04 Weakness/tiredness general code.
For ICPC-3, there are two new codes: AS05 Postviral fatigue and its Inclusion AS05.00 Chronic fatigue syndrome which are listed under the "General" A codes. Myalgic encephalomyelitis is listed as an Index term to AS05. These terms are cross mapped to ICD-10 G93.3 and ICD-11 8E49.
There is an Exclusion under these two codes for ICPC-3's AS04 weakness/tiredness, general code.
The Descriptive text is execrable and needs comments and proposals for revision submitting by advocates, patient groups, clinical allies etc.)
Section A General
AS General symptoms, complaints and abnormal findings
AS05 Postviral fatigue
AS05.00 Chronic fatigue syndrome
AS05 Postviral fatigue
Description
Postviral fatigue is characterised by persistent or recurrent fatigue, diffuse musculoskeletal pain, sleep disturbances, and subjective cognitive impairment of 6 months duration or longer. Symptoms are not caused by ongoing exertion; are not relieved by rest; and result in a substantial reduction of previous levels of occupational, educational, social or personal activities. Minor alterations of immune, neuroendocrine, and autonomic function may be associated with postviral fatigue.
Chronic fatigue syndrome: considerable cultural variations occur in the presentation of this problem, and two main types occur, with substantial overlap. In one type, the main feature is a complaint of increased fatigue after mental effort, often associated with some decrease in occupational performance or coping efficiency in daily tasks. The mental fatiguability is typically described as an unpleasant intrusion of distracting associations or recollections, difficulty in concentrating, and generally inefficient thinking. In the other type, the emphasis is on feelings of bodily or physical weakness and exhaustion after only minimal effort, accompanied by a feeling of muscular aches and pains and inability to relax. In both types a variety of other unpleasant physical feelings is common, such as dizziness, tension headaches, and feelings of general instability. Worry about decreasing mental and bodily well-being, irritability, anhedonia, and varying minor degrees of both depression and anxiety are all common. Sleep is often disturbed in its initial and middle phases but hypersomnia may also be prominent.
Inclusion
chronic fatigue syndrome AS05.00
Exclusion
weakness/tiredness, general AS04
Index terms
chronic fatigue syndrome
myalgic encephalomyelitis
ICPC-1
A04
ICPC-2
A04
ICD10
Postviral fatigue syndrome G93.3
ICD11
Postviral fatigue syndrome 8E49
SNOMED CT
chronic fatigue syndrome = myalgic encephalomyelitis Id 52702003
postviral fatigue syndrome (disorder) Id 51771007
-------------------------------------------
This is the listing for "Bodily distress or somatisation disorder" in ICPC-3 (my comments in blue and in brackets):
Section P Psychological, mental and neurodevelopmental
PD Psychological, mental and neurodevelopmental diagnoses and diseases
PD10 Bodily distress or somatisation disorder
(New code PD10 Bodily distress or somatisation disorder replaces ICPC-2 code P75 Somatisation disorder.)
Description
Bodily distress disorder is characterised by the presence of bodily symptoms that are distressing to the individual and excessive attention directed toward the symptoms, which may be manifest by repeated contact with health care providers. If another health condition is causing or contributing to the symptoms, the degree of attention is clearly excessive in relation to its nature and progression. Excessive attention is not alleviated by appropriate clinical examination and investigations and appropriate reassurance. Bodily symptoms are persistent, being present on most days for at least several months. Typically, bodily distress disorder involves multiple bodily symptoms that may vary over time. Occasionally there is a single symptom, usually pain or fatigue, that is associated with the other features of the disorder.
(This Description text is identical to ICD-11's Description text for "Bodily distress disorder" apart from omission of the final sentence of ICD-11's BDD Description text, which reads:
"...The symptoms and associated distress and preoccupation have at least some impact on the individual’s functioning (e.g. strain in relationships, less effective academic or occupational functioning, abandonment of specific leisure activities)."
Inclusion
somatization disorder
Index terms
bodily distress disorder
conversion disorder (This term does not align with ICD-11 which classifies "Dissociative neurological symptom disorder" - the ICD-11 equivalent of "conversion disorder" - under Dissociative disorders, not under BDD.)
pseudocyesis (This term is coded to F45.8 in ICD-10. "Pseudocyesis" [phantom pregnancy] is not included in ICD-11, as far as I can determine.)
somatic symptom [sic] (I think this should read "somatic symptom disorder" if they intend to align with ICD-11's list of Synonyms terms under BBD.)
somatoform disorder
(They have omitted ICD-11's list of exclusion terms, which includes excludes for PVFS, ME; and CFS under BDD.)
ICPC-1
P75
ICPC-2
P75
ICD10
no exact coresponding [sic] class 00
Somatization disorder F45.0
Undifferentiated somatoform disorder F45.1
ICD11
Bodily distress disorder 6C20
SNOMED CT
bodily distress disorder Id 723916001
somatization disorder Id 397923000
somatoform disorder Id 31297008
------------------------------------
It appears that the developers of ICPC-3 have chosen to revise ICPC-2's P75 term to align with ICD-11's Bodily distress disorder construct and have not included Fink's BDS term and disorder construct within the revised classification, as far as I can see; they are cross mapping code PD10 Bodily distress or somatisation disorder to ICD-11's 6C20 Bodily distress disorder, and to SNOMED CT's 723916001 Bodily distress disorder.
As I say, I am not intending to comment on the content of ICPC-3 or submit proposals for improvements since I am retired, but I would urge advocates and patient groups to submit for improvements, particularly in those countries which currently use ICPC-2 in primary care (Denmark, Netherlands and others).
Edited for clarity and to insert image
Last edited:
Dx Revision Watch
Senior Member (Voting Rights)
Update to: IAPT requests code for Somatic symptom disorder for SNOMED CT
Last November, I posted links for 9 documents in Post #453 which included a report on the status of IAPT leads' November 2019 request for addition of a Concept code that is "the equivalent of Somatic Symptom Disorder in DSM-5" to the UK Edition of SNOMED CT terminology system [1].
IAPT leads submitted this request in order that they might use the term "Somatic symptom disorder" in the new IAPT Data Set v2.0.
Data Set v2.0 requires the availability of an ICD-10 code or a Concept code from the SNOMED CT UK Edition terminology system for use in records, data submission and statistical analysis. There is no code for "Somatic symptom disorder" in ICD-10.
IAPT's intention was to replace the Data Set v1.5 terminology, "MUS - not otherwise specified" (a term IAPT now considers no longer appropriate for that cohort) with the term, "Somatic symptom disorder" for Data Set v2.0, which was rolled out last September*.
According to the brief rationale supporting Request ID 29847: "The IAPT National Clinical Advisor highlighted that Somatic Symptom Disorder . . . in DSM-5 is the appropriate definition for this cohort."
*The roll-out date for Data Set v2.0 had originally been scheduled for April 2020 and IAPT had hoped to fast track this request in time for inclusion in SNOMED CT UK Edition's April 2020 release.
For the background to this request see:
IAPT requests code for Somatic symptom disorder for SNOMED CT, November 2020 [2]:
https://bit.ly/3fLpEVL
In February 2020, I wrote to NHS Digital's terminology and classification leads advocating against the addition of a Somatic symptom disorder term to the SNOMED CT UK Edition.
In March 2020, I was advised by NHS Digital that discussions were still ongoing and no decision had been reached.
In June 2020, NHS Digital updated that no decision had been reached and further research and discussions were taking place with SNOMED International.
In July 2020, I was informed that as there is an existing international concept 723916001 Bodily distress disorder in SNOMED CT [which corresponds conceptually to ICD-11's Bodily distress disorder*] and as ICD-11 lists Somatic symptom disorder under synonyms under 6C20 Bodily distress disorder, Request ID 29847 had been referred to SNOMED International for review and processing.
If SNOMED International were to approve the authoring of a unique concept code for Somatic symptom disorder for inclusion in the International Edition or add the term under synonyms to SNOMED CT's existing 723916001 Bodily distress disorder concept for congruency with WHO's ICD-11, its addition to the terminology system would subsequently be absorbed by the UK Edition and the various national extensions.
*In ICD-11, there are exclusions for PVFS; ME; and CFS under 6C20 Bodily distress disorder.
Update:
SNOMED International has approved the addition of Somatic symptom disorder under Synonyms to existing Concept code, 723916001 Bodily distress disorder.
This decision was implemented for the International Edition's January 31, 2021 release. The addition of this Synonyms term to the International Edition was absorbed by the UK Edition's May 12, 2021 release.
Concept code 723916001 is mapped to F45.9 Somatoform disorder, unspecified in the SNOMED CT UK to ICD-10 Classification Map.
A revised version of spreadsheet IAPT v2.0 Terminology Mapping Guidance has been posted on the "Submitting IAPT data" page incorporating this term [3][4]:
IAPT v2.0 Terminology Mapping Guidance v3.4 25 May 2021
Mapping Guidance for Data Set v1.5 flow to Data Set v2.0:
Note:
Irritable Bowel Syndrome coded to ICD-10 K58.0 and K58.0
Chronic fatigue syndromes/Myalgic encephalopathy (ME) [sic] coded to ICD-10 G93.3
MUS - not otherwise specified coded to SNOMED CT 723916001 Somatic symptom disorder
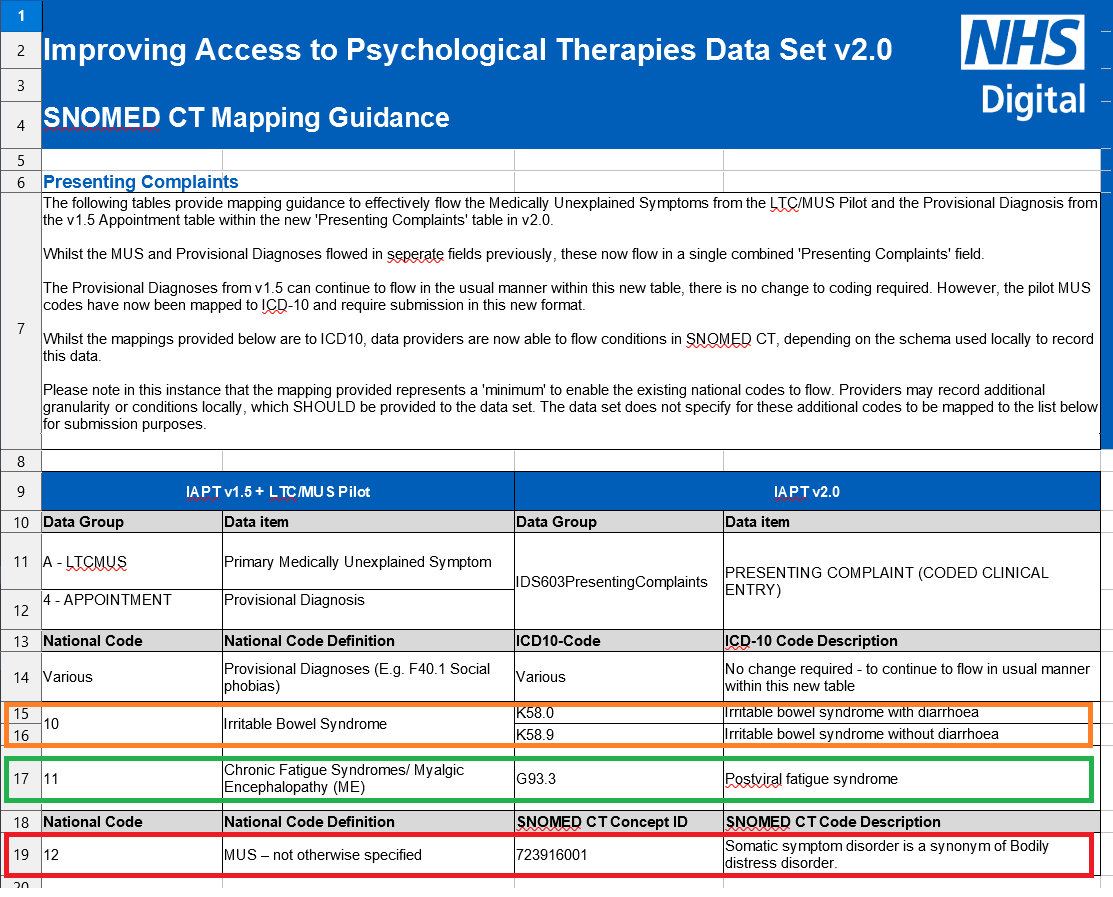
So although IAPT leads did not obtain the creation of a unique SNOMED CT Concept code for the term, Somatic symptom disorder, there is now a SNOMED CT Synonyms term coded under 723916001 available for use in IAPT Data Set v2.0 and its associated documentation.
I remain very concerned that embedding the Somatic symptom disorder term and code within IAPT may result in seepage of the SSD term beyond IAPT's use, with the potential for its wider application within NHS England primary and secondary care settings and mental health settings.
Eventually, the ICD-11 6C20 Bodily distress disorder code will be available to NHS England.
With regard to adoption and migration to ICD-11, NHS Digital has stated: "No decision has been made for the implementation of ICD-11 in England, however NHS Digital plan to undertake further testing of the latest release and supporting products that will inform a future decision."
The mandated version of ICD-10 for use in NHS England remains ICD-10 Version: 2016. It is not yet confirmed whether NHS Digital intends to implement ICD-10 Version: 2019 or skip the final release of ICD-10 in preference to migrating directly to ICD-11, at some point in the next few years.
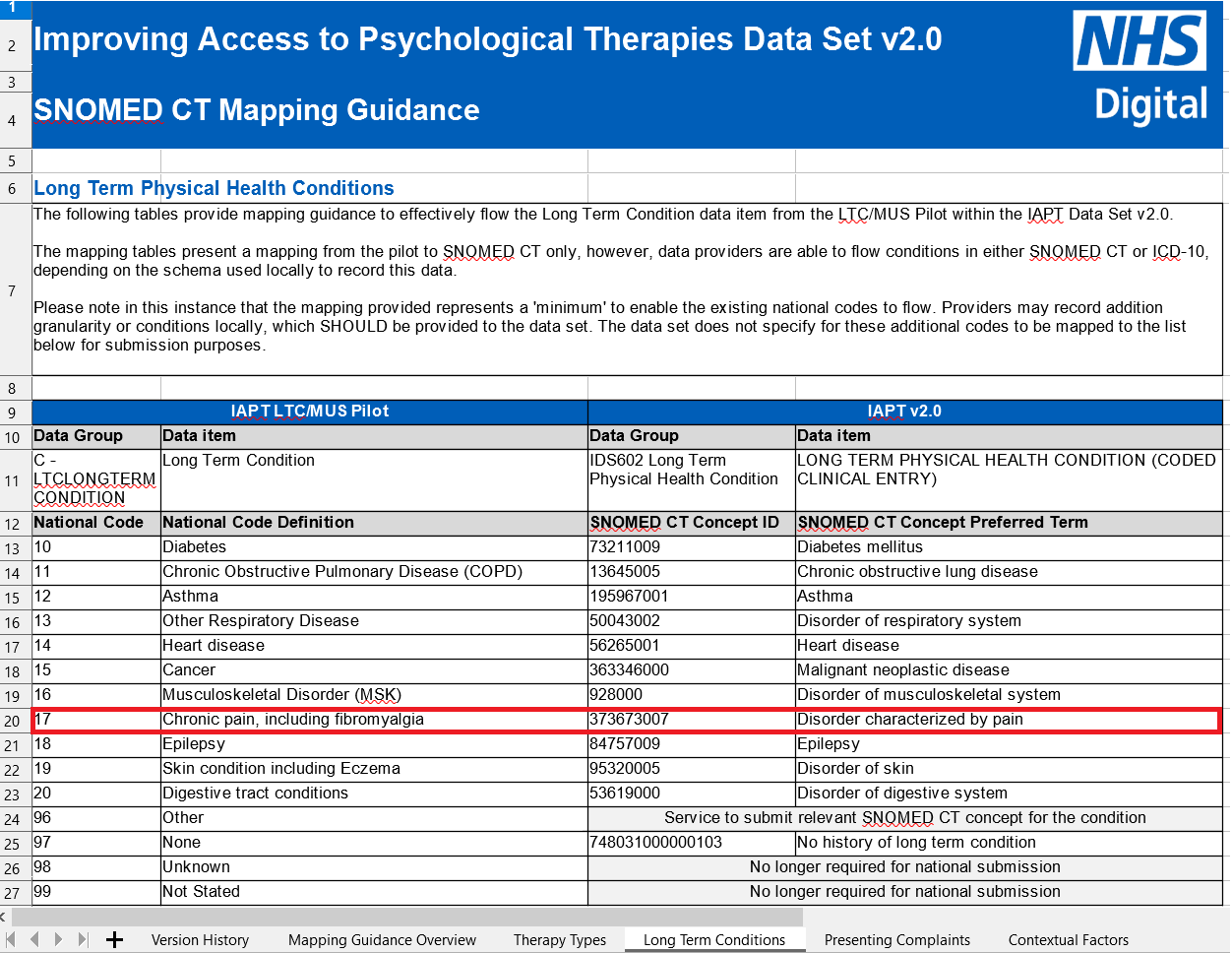
Here is the IAPT Data Set v2.0 Mapping Guidance for Long Term Physical Health Conditions, which includes Chronic pain and Fibromyalgia:
IAPT v2.0 Terminology Mapping Guidance v3.4 25 May 2021
References:
1 SNOMED CT Submission Portal Request ID 29847, submitted on behalf of IAPT, November 2019:
https://isd.hscic.gov.uk/rsp-snomed/user/guest/request/view.jsf?request_id=29847
2 For the background to this request:
IAPT requests code for Somatic symptom disorder for SNOMED CT, Suzy Chapman, November 2020:
https://dxrevisionwatch.files.wordp...or-somatic-symptom-disorder-for-snomed-ct.pdf
3 Submitting IAPT data: https://digital.nhs.uk/data-and-inf...gical-therapies-data-set/submitting-iapt-data
4 Revised spreadsheet: IAPT v2.0 Terminology Mapping Guidance v3.4, 25 May 2021
https://nhs-prod.global.ssl.fastly....apt_v2_terminology_mapping_guidance_v3.4.xlsx
Minor edits to include an additional para and link.
Edited to add:
This information has been included in the July edition of NHS Digital's Mental Health Information Update newsletter:
Last November, I posted links for 9 documents in Post #453 which included a report on the status of IAPT leads' November 2019 request for addition of a Concept code that is "the equivalent of Somatic Symptom Disorder in DSM-5" to the UK Edition of SNOMED CT terminology system [1].
IAPT leads submitted this request in order that they might use the term "Somatic symptom disorder" in the new IAPT Data Set v2.0.
Data Set v2.0 requires the availability of an ICD-10 code or a Concept code from the SNOMED CT UK Edition terminology system for use in records, data submission and statistical analysis. There is no code for "Somatic symptom disorder" in ICD-10.
IAPT's intention was to replace the Data Set v1.5 terminology, "MUS - not otherwise specified" (a term IAPT now considers no longer appropriate for that cohort) with the term, "Somatic symptom disorder" for Data Set v2.0, which was rolled out last September*.
According to the brief rationale supporting Request ID 29847: "The IAPT National Clinical Advisor highlighted that Somatic Symptom Disorder . . . in DSM-5 is the appropriate definition for this cohort."
*The roll-out date for Data Set v2.0 had originally been scheduled for April 2020 and IAPT had hoped to fast track this request in time for inclusion in SNOMED CT UK Edition's April 2020 release.
For the background to this request see:
IAPT requests code for Somatic symptom disorder for SNOMED CT, November 2020 [2]:
https://bit.ly/3fLpEVL
In February 2020, I wrote to NHS Digital's terminology and classification leads advocating against the addition of a Somatic symptom disorder term to the SNOMED CT UK Edition.
In March 2020, I was advised by NHS Digital that discussions were still ongoing and no decision had been reached.
In June 2020, NHS Digital updated that no decision had been reached and further research and discussions were taking place with SNOMED International.
In July 2020, I was informed that as there is an existing international concept 723916001 Bodily distress disorder in SNOMED CT [which corresponds conceptually to ICD-11's Bodily distress disorder*] and as ICD-11 lists Somatic symptom disorder under synonyms under 6C20 Bodily distress disorder, Request ID 29847 had been referred to SNOMED International for review and processing.
If SNOMED International were to approve the authoring of a unique concept code for Somatic symptom disorder for inclusion in the International Edition or add the term under synonyms to SNOMED CT's existing 723916001 Bodily distress disorder concept for congruency with WHO's ICD-11, its addition to the terminology system would subsequently be absorbed by the UK Edition and the various national extensions.
*In ICD-11, there are exclusions for PVFS; ME; and CFS under 6C20 Bodily distress disorder.
Update:
SNOMED International has approved the addition of Somatic symptom disorder under Synonyms to existing Concept code, 723916001 Bodily distress disorder.
This decision was implemented for the International Edition's January 31, 2021 release. The addition of this Synonyms term to the International Edition was absorbed by the UK Edition's May 12, 2021 release.
Concept code 723916001 is mapped to F45.9 Somatoform disorder, unspecified in the SNOMED CT UK to ICD-10 Classification Map.
A revised version of spreadsheet IAPT v2.0 Terminology Mapping Guidance has been posted on the "Submitting IAPT data" page incorporating this term [3][4]:
IAPT v2.0 Terminology Mapping Guidance v3.4 25 May 2021
Mapping Guidance for Data Set v1.5 flow to Data Set v2.0:
Note:
Irritable Bowel Syndrome coded to ICD-10 K58.0 and K58.0
Chronic fatigue syndromes/Myalgic encephalopathy (ME) [sic] coded to ICD-10 G93.3
MUS - not otherwise specified coded to SNOMED CT 723916001 Somatic symptom disorder
So although IAPT leads did not obtain the creation of a unique SNOMED CT Concept code for the term, Somatic symptom disorder, there is now a SNOMED CT Synonyms term coded under 723916001 available for use in IAPT Data Set v2.0 and its associated documentation.
I remain very concerned that embedding the Somatic symptom disorder term and code within IAPT may result in seepage of the SSD term beyond IAPT's use, with the potential for its wider application within NHS England primary and secondary care settings and mental health settings.
Eventually, the ICD-11 6C20 Bodily distress disorder code will be available to NHS England.
With regard to adoption and migration to ICD-11, NHS Digital has stated: "No decision has been made for the implementation of ICD-11 in England, however NHS Digital plan to undertake further testing of the latest release and supporting products that will inform a future decision."
The mandated version of ICD-10 for use in NHS England remains ICD-10 Version: 2016. It is not yet confirmed whether NHS Digital intends to implement ICD-10 Version: 2019 or skip the final release of ICD-10 in preference to migrating directly to ICD-11, at some point in the next few years.
Here is the IAPT Data Set v2.0 Mapping Guidance for Long Term Physical Health Conditions, which includes Chronic pain and Fibromyalgia:
IAPT v2.0 Terminology Mapping Guidance v3.4 25 May 2021
References:
1 SNOMED CT Submission Portal Request ID 29847, submitted on behalf of IAPT, November 2019:
https://isd.hscic.gov.uk/rsp-snomed/user/guest/request/view.jsf?request_id=29847
2 For the background to this request:
IAPT requests code for Somatic symptom disorder for SNOMED CT, Suzy Chapman, November 2020:
https://dxrevisionwatch.files.wordp...or-somatic-symptom-disorder-for-snomed-ct.pdf
3 Submitting IAPT data: https://digital.nhs.uk/data-and-inf...gical-therapies-data-set/submitting-iapt-data
4 Revised spreadsheet: IAPT v2.0 Terminology Mapping Guidance v3.4, 25 May 2021
https://nhs-prod.global.ssl.fastly....apt_v2_terminology_mapping_guidance_v3.4.xlsx
Minor edits to include an additional para and link.
Edited to add:
This information has been included in the July edition of NHS Digital's Mental Health Information Update newsletter:
https://elinkeu.clickdimensions.com/m/1/58255379/p1-t21181-34d3497967844a739a7e9f6e6cbf889a/1/1/1
Introduction
This regular update includes the latest information and relevant updates on all mental health data sets that we collect and report.
(...)
IAPT Terminology Mapping Guidance – code for Somatic Symptom Disorder
Following the recent SNOMED CT release, the IAPT Terminology Mapping Guidance has been updated with the SNOMED CT code to enable mapping from ‘MUS – not otherwise specified’ to ‘Somatic Symptom Disorder’, a synonym of Bodily Distress Disorder. To view the mapping document, please visit https://digital.nhs.uk/data-and-inf...gical-therapies-data-set/submitting-iapt-data
Introduction
This regular update includes the latest information and relevant updates on all mental health data sets that we collect and report.
(...)
IAPT Terminology Mapping Guidance – code for Somatic Symptom Disorder
Following the recent SNOMED CT release, the IAPT Terminology Mapping Guidance has been updated with the SNOMED CT code to enable mapping from ‘MUS – not otherwise specified’ to ‘Somatic Symptom Disorder’, a synonym of Bodily Distress Disorder. To view the mapping document, please visit https://digital.nhs.uk/data-and-inf...gical-therapies-data-set/submitting-iapt-data
Last edited:
Wyva
Senior Member (Voting Rights)
Thank you for informing us of all this, it is very useful, @Dx Revision Watch
I may be off-topic but I started digging around a bit to see what's going on with other diseases that get mentioned a lot on this forum. Here is what I found if someone's interested:
1. In ICD-10 (I'm looking at the 2019 version) fibromyalgia has the code M79.7, in the category of Diseases of the musculoskeletal system and connective tissue, more specifically in Other soft tissue disorders, not elsewhere classified. https://icd.who.int/browse10/2019/en#/M79.7
In the upcoming ICD-11 the code is now MG30.01 Chronic widespread pain and the name fibromyalgia is listed as an inclusion. The main category is Symptoms, signs or clinical findings, not elsewhere classified and within that: General symptoms, signs or clinical findings and finally the Pain and Chronic pain categories. (You can also use additional codes to specify, for example to note if there are psychosocial factors present or not.) This kind of looks like a "downgrade" to me.
https://icd.who.int/browse11/l-m/en#/http://id.who.int/icd/entity/849253504
2. Irritable bowel syndrome was originally listed in the category Diseases of the digestive system and within that in the category Other diseases of intestines. https://icd.who.int/browse10/2019/en#/K58
In ICD-11, it will be DD91.0 Irritable bowel syndrome in the category Functional gastrointestinal disorders and will stay in the same main category (digestive). https://icd.who.int/browse11/l-m/en#/http://id.who.int/icd/entity/1158238623
3. There was no specific code for POTS in ICD-10, but now there is one on ICD-11: 8D89.2 Postural orthostatic tachycardia syndrome, in the category of Disorders of orthostatic tolerance, within Disorders of autonomic nervous system, while the main category is Diseases of the nervous system. https://icd.who.int/browse11/l-m/en#/http://id.who.int/icd/entity/1533647472
4. No sign of mast cell activation syndrome.
I may be off-topic but I started digging around a bit to see what's going on with other diseases that get mentioned a lot on this forum. Here is what I found if someone's interested:
1. In ICD-10 (I'm looking at the 2019 version) fibromyalgia has the code M79.7, in the category of Diseases of the musculoskeletal system and connective tissue, more specifically in Other soft tissue disorders, not elsewhere classified. https://icd.who.int/browse10/2019/en#/M79.7
In the upcoming ICD-11 the code is now MG30.01 Chronic widespread pain and the name fibromyalgia is listed as an inclusion. The main category is Symptoms, signs or clinical findings, not elsewhere classified and within that: General symptoms, signs or clinical findings and finally the Pain and Chronic pain categories. (You can also use additional codes to specify, for example to note if there are psychosocial factors present or not.) This kind of looks like a "downgrade" to me.
https://icd.who.int/browse11/l-m/en#/http://id.who.int/icd/entity/849253504
2. Irritable bowel syndrome was originally listed in the category Diseases of the digestive system and within that in the category Other diseases of intestines. https://icd.who.int/browse10/2019/en#/K58
In ICD-11, it will be DD91.0 Irritable bowel syndrome in the category Functional gastrointestinal disorders and will stay in the same main category (digestive). https://icd.who.int/browse11/l-m/en#/http://id.who.int/icd/entity/1158238623
3. There was no specific code for POTS in ICD-10, but now there is one on ICD-11: 8D89.2 Postural orthostatic tachycardia syndrome, in the category of Disorders of orthostatic tolerance, within Disorders of autonomic nervous system, while the main category is Diseases of the nervous system. https://icd.who.int/browse11/l-m/en#/http://id.who.int/icd/entity/1533647472
4. No sign of mast cell activation syndrome.
Dx Revision Watch
Senior Member (Voting Rights)
In the upcoming ICD-11 the code is now MG30.01 Chronic widespread pain and the name fibromyalgia is listed as an inclusion. The main category is Symptoms, signs or clinical findings, not elsewhere classified and within that: General symptoms, signs or clinical findings and finally the Pain and Chronic pain categories. (You can also use additional codes to specify, for example to note if there are psychosocial factors present or not.) This kind of looks like a "downgrade" to me.
https://icd.who.int/browse11/l-m/en#/http://id.who.int/icd/entity/849253504
Indeed.
Fibromyalgia (or "Fibromyalgia syndrome", as it is now listed in ICD-11) has lost its discrete code for ICD-11's equivalent to the Tabular List.
"Fibromyalgia syndrome" Description text is here: https://icd.who.int/dev11/f/en#http://id.who.int/icd/entity/236601102
In May 2015, Fibromyalgia was very quietly deleted from the Beta draft's Diseases of the musculoskeletal system or connective tissue chapter and relocated to the Symptoms, signs chapter Chronic primary pain disorder block.
This change of chapter should have first been submitted for public review via the ICD-11 Proposal Mechanism - but it wasn't.
There have been no comments about this relocation from FM stakeholder patient organizations, the clinicians who advise them, allied health professionals, disability lawyers etc. Several FM patient advocacy orgs have been given the information they need to provide feedback or suggest improvements - but haven't done so.
The development of a new Chronic pain and Chronic primary pain category block for ICD-11 has been the responsibility of the IASP Task Force.
In 2013, the International Association for the Study of Pain (IASP) established a Task Force for the development of the classification of Chronic Pain and Chronic primary pain and has worked in collaboration with ICD Revision.
In the IASP's original 2015 position paper, the group was recommending shifting all three terms, Fibromyalgia, Chronic widespread pain and IBS under this new Chronic primary pain category block:
Treede, R. D., Rief, W., Barke, A., Aziz, Q., Bennett, M. I., Benoliel, R., Cohen, M., Evers, S., Finnerup, N. B., First, M. B., Giamberardino, M. A., Kaasa, S., Kosek, E., Lavand'homme, P., Nicholas, M., Perrot, S., Scholz, J., Schug, S., Smith, B. H., Svensson, P., … Wang, S. J. (2015). A classification of chronic pain for ICD-11. Pain, 156(6), 1003–1007. https://doi.org/10.1097/j.pain.0000000000000160
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4450869/
"2.1. Chronic primary pain
Chronic primary pain is pain in 1 or more anatomic regions that persists or recurs for longer than 3 months and is associated with significant emotional distress or significant functional disability (interference with activities of daily life and participation in social roles) and that cannot be better explained by another chronic pain condition. This is a new phenomenological definition, created because the etiology is unknown for many forms of chronic pain. Common conditions such as, eg, back pain that is neither identified as musculoskeletal or neuropathic pain, chronic widespread pain, fibromyalgia, and irritable bowel syndrome will be found in this section and biological findings contributing to the pain problem may or may not be present. The term “primary pain” was chosen in close liaison with the ICD-11 revision committee, who felt this was the most widely acceptable term, in particular, from a nonspecialist perspective..."
and under 2.7. Chronic musculoskeletal pain:
"…Well-described apparent musculoskeletal conditions for which the causes are incompletely understood, such as nonspecific back pain or chronic widespread pain, will be included in the section on chronic primary pain."
There were several formal submissions on behalf of the IASP Task Force for relocating IBS under this new Chronic primary pain block. But ICD Revision rejected these proposals and IBS has remained under the Diseases of the digestive system chapter, albeit under the parent, Functional gastrointestinal disorders.https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4450869/
"2.1. Chronic primary pain
Chronic primary pain is pain in 1 or more anatomic regions that persists or recurs for longer than 3 months and is associated with significant emotional distress or significant functional disability (interference with activities of daily life and participation in social roles) and that cannot be better explained by another chronic pain condition. This is a new phenomenological definition, created because the etiology is unknown for many forms of chronic pain. Common conditions such as, eg, back pain that is neither identified as musculoskeletal or neuropathic pain, chronic widespread pain, fibromyalgia, and irritable bowel syndrome will be found in this section and biological findings contributing to the pain problem may or may not be present. The term “primary pain” was chosen in close liaison with the ICD-11 revision committee, who felt this was the most widely acceptable term, in particular, from a nonspecialist perspective..."
and under 2.7. Chronic musculoskeletal pain:
"…Well-described apparent musculoskeletal conditions for which the causes are incompletely understood, such as nonspecific back pain or chronic widespread pain, will be included in the section on chronic primary pain."
The IASP Task Force later proposed that IBS should be secondary parented to the new Chronic primary pain block. Again, this proposal was rejected by ICD-Revision.
Prof Winfried Rief is a member of the IASP Task Force.
In this Rief presentation dating from 2012, Rief was suggesting that for ICD-11, Chronic fatigue syndrome might be one of several "Potential partners in a new chapter: (Other) functional somatic conditions"
Slide #15:
Potential partners in a new chapter:
(Other) functional somatic conditions
V.1 Multiple Bodily Distress Disorder
V.2 Complex Irritable Bowel Syndrome (IBS with associated psychological features)
V.3 Chronic Fatigue Syndrome, Neurasthenia
V.31 Chronic Fatigue in the context of Cancer
V.4 Environmental Sensitivity Syndromes
V.5 Health anxiety disorder
V.9 Other Bodily Distress Disorders -> Overlap of symptoms,
several psychological and biological mechanisms
Potential partners in a new chapter:
(Other) functional somatic conditions
V.1 Multiple Bodily Distress Disorder
V.2 Complex Irritable Bowel Syndrome (IBS with associated psychological features)
V.3 Chronic Fatigue Syndrome, Neurasthenia
V.31 Chronic Fatigue in the context of Cancer
V.4 Environmental Sensitivity Syndromes
V.5 Health anxiety disorder
V.9 Other Bodily Distress Disorders -> Overlap of symptoms,
several psychological and biological mechanisms
Rief had also floated the potential for creating a new chapter for ICD-11 specifically for Pain categories.
Presentation: IASP and the Classification of Pain in ICD-11, Prof. Dr. Winfried Rief, University of Marburg, Germany:
PDF: https://dxrevisionwatch.files.wordp...ied-rief_copenhagen-efic-pain-rief-2012-3.pdf
This new Chronic pain and Chronic primary pain block in the ICD-11 Symptoms, signs chapter contains a good deal of psychosomatics and expands conceptually on ICD-10's F45.4 Persistent somatoform pain disorder.
Before the ICD-11 Beta draft was approved by the WHA in May 2019, the IASP had also suggested (informally and not through the official Proposal Mechanism platform), that ICD-11's 6C20 Bodily distress disorder should be secondary parented to the new Chronic primary pain category block. This has not been actioned by WHO/ICD Revision. There is considerable conceptual overlap between Bodily distress disorder and these new Chronic primary pain disorder categories.
Last edited:
Dx Revision Watch
Senior Member (Voting Rights)
Update to: IAPT requests code for Somatic symptom disorder for SNOMED CT
(...)
SNOMED International has approved the addition of Somatic symptom disorder under Synonyms to existing Concept code, 723916001 Bodily distress disorder.
This decision was implemented for the International Edition's January 31, 2021 release. The addition of this Synonyms term to the International Edition was absorbed by the UK Edition's May 12, 2021 release.
The SNOMED CT International Edition, a Spanish Edition, and browsers for 14 national editions can be accessed at: https://browser.ihtsdotools.org/
The following SNOMED CT national editions have now also absorbed "Somatic symptom disorder" under Synonyms under 723916001 Bodily distress disorder:
Argentinian Edition (under 723916001: Trastorno de sufrimiento corporal)
Belgium Edition
Canadian Edition
Danish Edition
Estonian Edition
Irish Edition
Netherlands Edition
New Zealand Edition
Swedish Edition
United States Edition
The remaining national editions that are publicly available via the SNOMED CT International Browser platform namely, Australia, Norway and Uruguay, have yet to post updated releases for 2021.
The next International Edition release is scheduled for July 31.
Dx Revision Watch
Senior Member (Voting Rights)
While I'm here...
The FY 2022 release of the U.S.'s ICD-10-CM "clinical modification" has just been posted on the CDC site.
The 2022 ICD-10-CM codes are to be used from October 1, 2021 through September 30, 2022 and will replace the FY 2021 January release.
https://cdc.gov/nchs/icd/icd10cm.htm
The following files are currently available:
As always, the CDC bundles most of these release files into Zip files, though latterly the Guidelines document has been posted as a separate PDF.
Note that the PDFs for the FY 2022 Tabular List and the Alphabetical Index are large files.
For ease of access, I have posted copies of the Tabular List PDF and the Index PDF on my site. Please note the file sizes if you intend to download these files:
ICD-10-CM FY 2022:
PDF: Tabular List [29MB file]:
https://dxrevisionwatch.files.wordpress.com/2021/06/icd10cm-tabular-2022.pdf
PDF: Index [41MG file]:
https://dxrevisionwatch.files.wordpress.com/2021/06/icd10cm-index-2022.pdf
I am disappointed to see that the ICD-10-CM FY 2022 Release has not absorbed the removal of the "Benign" prefix from "Benign myalgic encephalomyelitis" - a change that was implemented for the final update of the WHO's International version of ICD-10 (ICD-10 Version: 2019), which the WHO released in January 2020.
The WHO-FIC ICD-10 Update & Revision Committee (URC) had approved this request in September 2016 for implementation in ICD-10 after January 2018:
Report:
World Health Organization removes "Benign" from "Benign myalgic encephalomyelitis" for ICD-11
https://dxrevisionwatch.files.wordpress.com/2020/11/world-health-organization-removes-benign-from-benign-myalgic-encephalomyelitis.pdf
CDC's Donna Pickett would have been a member of the WHO-FIC ICD-10 Update & Revision Committee that approved this change, back in 2016.
There may be legitimate reasons why this terminology revision to the International edition of ICD-10 has not been incorporated into the FY 2022 ICD-10-CM release. Possibly because of C-19, not all revisions to the WHO's ICD-10 version are being absorbed this year - but I don't know.
I have not been involved in the advocacy around the incorporation of this change into ICD-10-CM and I'm not up to speed with the reason(s) behind this change not having been incorporated into the FY 2022 release.
The twice yearly public ICD-10-CM Coordination and Maintenance Committee meetings have been held virtually since March 2020 and I have not been following the recordings since the March 17-18, 2020 virtual meeting.
The status of incorporation of revisions to the WHO's ICD-10 International version may have been clarified within the meeting recordings or in the "housekeeping" sections at the beginning of the public meeting Topic Packet documents.
So the U.S.'s FY 2022 Tabular List entry for G93.3 still remains as:
and I cannot see a term for "myalgic encephalomyelitis" (ie without the "Benign" prefix) listed in the Index, either.
*Edited to insert:
The ICD-10-CM Official Guidelines for Coding and Reporting FY 2022 (October 1, 2021 - September 30, 2022) document is now available:
https://ftp.cdc.gov/pub/Health_Stat...0CM/2022/10cmguidelines-FY2022-7-2022-508.pdf
The FY 2022 release of the U.S.'s ICD-10-CM "clinical modification" has just been posted on the CDC site.
The 2022 ICD-10-CM codes are to be used from October 1, 2021 through September 30, 2022 and will replace the FY 2021 January release.
https://cdc.gov/nchs/icd/icd10cm.htm
The following files are currently available:
- ICD-10-CM FY2021 Full PDF 2022
- ICD-10-CM FY2021 XML 2022
- ICD-10-CM FY 2021 Addenda PDF 2022
- ICD-10-CM FY 2021 List of codes and Descriptions 2022
- ICD-10-CM FY2021 Order Files 2022
- ICD-10-CM FY2021 Conversion Table 2022
As always, the CDC bundles most of these release files into Zip files, though latterly the Guidelines document has been posted as a separate PDF.
Note that the PDFs for the FY 2022 Tabular List and the Alphabetical Index are large files.
For ease of access, I have posted copies of the Tabular List PDF and the Index PDF on my site. Please note the file sizes if you intend to download these files:
ICD-10-CM FY 2022:
PDF: Tabular List [29MB file]:
https://dxrevisionwatch.files.wordpress.com/2021/06/icd10cm-tabular-2022.pdf
PDF: Index [41MG file]:
https://dxrevisionwatch.files.wordpress.com/2021/06/icd10cm-index-2022.pdf
I am disappointed to see that the ICD-10-CM FY 2022 Release has not absorbed the removal of the "Benign" prefix from "Benign myalgic encephalomyelitis" - a change that was implemented for the final update of the WHO's International version of ICD-10 (ICD-10 Version: 2019), which the WHO released in January 2020.
The WHO-FIC ICD-10 Update & Revision Committee (URC) had approved this request in September 2016 for implementation in ICD-10 after January 2018:
Report:
World Health Organization removes "Benign" from "Benign myalgic encephalomyelitis" for ICD-11
https://dxrevisionwatch.files.wordpress.com/2020/11/world-health-organization-removes-benign-from-benign-myalgic-encephalomyelitis.pdf
CDC's Donna Pickett would have been a member of the WHO-FIC ICD-10 Update & Revision Committee that approved this change, back in 2016.
There may be legitimate reasons why this terminology revision to the International edition of ICD-10 has not been incorporated into the FY 2022 ICD-10-CM release. Possibly because of C-19, not all revisions to the WHO's ICD-10 version are being absorbed this year - but I don't know.
I have not been involved in the advocacy around the incorporation of this change into ICD-10-CM and I'm not up to speed with the reason(s) behind this change not having been incorporated into the FY 2022 release.
The twice yearly public ICD-10-CM Coordination and Maintenance Committee meetings have been held virtually since March 2020 and I have not been following the recordings since the March 17-18, 2020 virtual meeting.
The status of incorporation of revisions to the WHO's ICD-10 International version may have been clarified within the meeting recordings or in the "housekeeping" sections at the beginning of the public meeting Topic Packet documents.
So the U.S.'s FY 2022 Tabular List entry for G93.3 still remains as:
G93.3 Postviral fatigue syndrome
Benign myalgic encephalomyelitis
Excludes1: chronic fatigue syndrome NOS (R53.82)
Excludes1: chronic fatigue syndrome NOS (R53.82)
and I cannot see a term for "myalgic encephalomyelitis" (ie without the "Benign" prefix) listed in the Index, either.
*Edited to insert:
The ICD-10-CM Official Guidelines for Coding and Reporting FY 2022 (October 1, 2021 - September 30, 2022) document is now available:
https://ftp.cdc.gov/pub/Health_Stat...0CM/2022/10cmguidelines-FY2022-7-2022-508.pdf
Last edited:
Dx Revision Watch
Senior Member (Voting Rights)
Re: ICPC-3:
Having fought long and hard for exclusions for the three 8E49 terms under ICD-11's MG22 Fatigue and 6C20 Bodily distress disorder I remain invested in seeing similar exclusions added for ICPC-3.
In ICPC-3, there is already an exclusion for AS04 weakness/tiredness, general under new code, AS05 Postviral fatigue, which is consistent with the exclusion of MG22 Fatigue under ICD-11's 8E49 Postviral fatigue syndrome - and welcomed.
But there is currently no reciprocal exclusion for the three terms under AS04 General weakness or tiredness and there is no exclusion for the three terms under PD10 Bodily distress or somatisation disorder, which do not accord with ICD-11.
Today and yesterday, I submitted proposals and brief rationales for some limited changes to the ICPC-3.
What I have submitted for are these changes:
1 That exclusions are added for
AS05 Postviral fatigue
AS05.00 chronic fatigue syndrome
myalgic encephalomyelitis
under code:
AS04 General weakness or tiredness
for consistency with ICD-11.
2 That exclusions are added for
AS05 Postviral fatigue
AS05.00 chronic fatigue syndrome
myalgic encephalomyelitis
under the new code:
PD10 Bodily distress or somatisation disorder
for consistency with ICD-11.
3 That the Index term "somatic symptom" [sic] under PD10 Bodily distress or somatisation disorder is corrected to "somatic symptom disorder" for consistency with ICD-11 terminology.
--------------------------------
What I won't be taking on is proposing and drafting rationales for the following:
1 That the ICPC-3 Description text for AS05 Postviral fatigue and AS05 Chronic fatigue syndrome needs urgent redrafting and provision of a draft text.
2 That myalgic encephalomyelitis is specified as an inclusion term under
AS05 Postviral fatigue
rather than being listed only as an Index term, for alignment with ICD-11 (or that all three terms are assigned a discrete sub code).
3 That the term, AS05 Postviral fatigue is revised to AS05 Postviral fatigue syndrome, for consistency with ICD-11 (or that a sub code for Postviral fatigue syndrome is added under AS05 Postviral fatigue.
4 That the three terms currently coded and indexed in ICPC-3 to AS05 and AS05.00 are moved from the ICPC-3 AS General symptoms, complaints and abnormal findings block and relocated under the ND Diagnoses and diseases of neurological system block, for consistency with their chapter location in ICD-11.
I have alerted Richard Simpson to the ICPC-3 development and proposal process and have also alerted the European ME Alliance group. I will be letting them know what proposals I have submitted and what proposals I cannot take on, due to my retirement.
Note that the ICPC-2 classification system is not mandated for use in NHS England and has more relevance for some EU countries. Some countries have developed national extensions and added additional sub codes.
According to this 2016 survey, a version of ICPC was available in a national language in 34 countries. ICPC was used in primary care settings in 27 countries and is a mandatory standard for use in primary care in 6 EU countries, (which includes the Netherlands):
Basílio N, Ramos C, Figueira S, Pinto D. Worldwide Usage of International
Classification of Primary Care use. Rev Bras Med Fam Comunidade. 2016;11(38):1-9. http://dx.doi.org/10.5712/rbmfc11(38)1225
PDF: https://docs.bvsalud.org/biblioref/2018/04/877826/1225-7879-3-pb.pdf
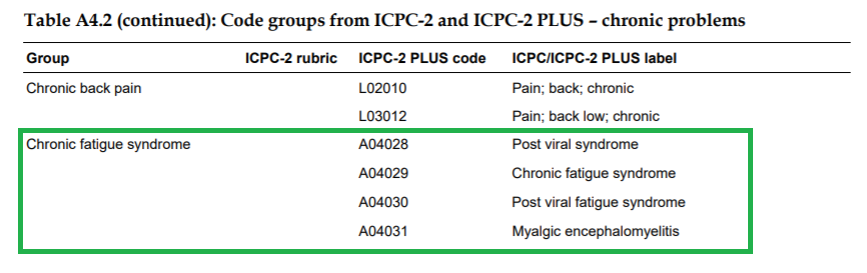
There is an Australian derivative of ICPC-2 known as ICPC-2 PLUS (also known as the BEACH coding system).
https://www.sydney.edu.au/medicine-...ifications-and-terminologies/icpc-2-plus.html
ICPC-2 PLUS is available under license and I don't have access to its codes.
But according to this document, Australia's ICPC-2 PLUS appears to include these additional codes to ICPC-2's A04 code:
https://ses.library.usyd.edu.au/bitstream/handle/2123/7772/Appendix 4.pdf
It is possibly too late to obtain changes prior to the finalisation of ICPC-3's book and e-book but changes might potentially be achieved for the first annual update (if they are submitted before June 2022).
It's not known how long it might take for early adopters of ICPC-3 to migrate to the new edition.
ICPC-3 landing page: https://www.icpc-3.info
ICPC-3 Browser: https://browser.icpc-3.info/index.php
Edited to include data from a 2016 survey: Worldwide Usage of International Classification of Primary Care use.
Having fought long and hard for exclusions for the three 8E49 terms under ICD-11's MG22 Fatigue and 6C20 Bodily distress disorder I remain invested in seeing similar exclusions added for ICPC-3.
In ICPC-3, there is already an exclusion for AS04 weakness/tiredness, general under new code, AS05 Postviral fatigue, which is consistent with the exclusion of MG22 Fatigue under ICD-11's 8E49 Postviral fatigue syndrome - and welcomed.
But there is currently no reciprocal exclusion for the three terms under AS04 General weakness or tiredness and there is no exclusion for the three terms under PD10 Bodily distress or somatisation disorder, which do not accord with ICD-11.
Today and yesterday, I submitted proposals and brief rationales for some limited changes to the ICPC-3.
What I have submitted for are these changes:
1 That exclusions are added for
AS05 Postviral fatigue
AS05.00 chronic fatigue syndrome
myalgic encephalomyelitis
under code:
AS04 General weakness or tiredness
for consistency with ICD-11.
2 That exclusions are added for
AS05 Postviral fatigue
AS05.00 chronic fatigue syndrome
myalgic encephalomyelitis
under the new code:
PD10 Bodily distress or somatisation disorder
for consistency with ICD-11.
3 That the Index term "somatic symptom" [sic] under PD10 Bodily distress or somatisation disorder is corrected to "somatic symptom disorder" for consistency with ICD-11 terminology.
--------------------------------
What I won't be taking on is proposing and drafting rationales for the following:
1 That the ICPC-3 Description text for AS05 Postviral fatigue and AS05 Chronic fatigue syndrome needs urgent redrafting and provision of a draft text.
2 That myalgic encephalomyelitis is specified as an inclusion term under
AS05 Postviral fatigue
rather than being listed only as an Index term, for alignment with ICD-11 (or that all three terms are assigned a discrete sub code).
3 That the term, AS05 Postviral fatigue is revised to AS05 Postviral fatigue syndrome, for consistency with ICD-11 (or that a sub code for Postviral fatigue syndrome is added under AS05 Postviral fatigue.
4 That the three terms currently coded and indexed in ICPC-3 to AS05 and AS05.00 are moved from the ICPC-3 AS General symptoms, complaints and abnormal findings block and relocated under the ND Diagnoses and diseases of neurological system block, for consistency with their chapter location in ICD-11.
I have alerted Richard Simpson to the ICPC-3 development and proposal process and have also alerted the European ME Alliance group. I will be letting them know what proposals I have submitted and what proposals I cannot take on, due to my retirement.
Note that the ICPC-2 classification system is not mandated for use in NHS England and has more relevance for some EU countries. Some countries have developed national extensions and added additional sub codes.
According to this 2016 survey, a version of ICPC was available in a national language in 34 countries. ICPC was used in primary care settings in 27 countries and is a mandatory standard for use in primary care in 6 EU countries, (which includes the Netherlands):
Basílio N, Ramos C, Figueira S, Pinto D. Worldwide Usage of International
Classification of Primary Care use. Rev Bras Med Fam Comunidade. 2016;11(38):1-9. http://dx.doi.org/10.5712/rbmfc11(38)1225
PDF: https://docs.bvsalud.org/biblioref/2018/04/877826/1225-7879-3-pb.pdf
There is an Australian derivative of ICPC-2 known as ICPC-2 PLUS (also known as the BEACH coding system).
https://www.sydney.edu.au/medicine-...ifications-and-terminologies/icpc-2-plus.html
"Primarily used in Australia, ICPC-2 PLUS is installed in various software packages and used in electronic health record (EHR) systems by approximately 6,000 GPs in more than 500 practices throughout Australia.
It is also used in research projects, including the BEACH (Bettering the Evaluation And Care of Health) program, the national study of general practice activity. The terminology is therefore often referred to as the BEACH coding system.
The terminology is maintained and regularly updated by the Classifications and terminologies node, WHO-CC for Strengthening Rehabilitation Capacity in Health Systems, University of Sydney. Users of ICPC-2 PLUS are actively involved in the ongoing development of the terminology."
It is also used in research projects, including the BEACH (Bettering the Evaluation And Care of Health) program, the national study of general practice activity. The terminology is therefore often referred to as the BEACH coding system.
The terminology is maintained and regularly updated by the Classifications and terminologies node, WHO-CC for Strengthening Rehabilitation Capacity in Health Systems, University of Sydney. Users of ICPC-2 PLUS are actively involved in the ongoing development of the terminology."
ICPC-2 PLUS is available under license and I don't have access to its codes.
But according to this document, Australia's ICPC-2 PLUS appears to include these additional codes to ICPC-2's A04 code:
https://ses.library.usyd.edu.au/bitstream/handle/2123/7772/Appendix 4.pdf
It is possibly too late to obtain changes prior to the finalisation of ICPC-3's book and e-book but changes might potentially be achieved for the first annual update (if they are submitted before June 2022).
It's not known how long it might take for early adopters of ICPC-3 to migrate to the new edition.
ICPC-3 landing page: https://www.icpc-3.info
ICPC-3 Browser: https://browser.icpc-3.info/index.php
Edited to include data from a 2016 survey: Worldwide Usage of International Classification of Primary Care use.
Last edited:
Simon M
Senior Member (Voting Rights)
Thanks, @Dx Revision Watch
As ever, I'm unable to read/follow everything you write but I am hugely appreciative of everything you're doing for the benefit of patients. Even more so as I realise you are now retired.
Thank you, from me and I suspect, everyone else here as well.
As ever, I'm unable to read/follow everything you write but I am hugely appreciative of everything you're doing for the benefit of patients. Even more so as I realise you are now retired.
Thank you, from me and I suspect, everyone else here as well.
Dx Revision Watch
Senior Member (Voting Rights)
Classification of Fibromyalgia for ICPC-3:
Fibromyalgia is also coded in ICPC-3 as an inclusion under Chronic widespread pain.
There is also a sub code for
LS18.00 primary fibromyalgia syndrome
https://browser.icpc-3.info/index.php
LS Symptoms, complaints and abnormal findings of musculoskeletal system
LS18 Chronic widespread pain
Description
Chronic widespread pain (CWP) is diffuse pain in at least 4 of 5 body regions and is associated with significant emotional distress (anxiety, anger/frustration or depressed mood) and functional disability (interference in daily life activities and reduced participation in social roles). CWP is multifactorial: biological, psychological and social factors contribute to the pain syndrome. The diagnosis is appropriate when the pain is not directly attributable to a nociceptive process in those regions and there are features consistent with nociplastic pain and identified psychological and social contributors. Other chronic pain diagnoses to be considered are chronic cancer pain, chronic postsurgical or posttraumatic pain, chronic neuropathic pain, chronic visceral pain and chronic musculoskeletal pain.
( ICD-11's Description text and Criteria for Chronic widespread pain is here: https://icd.who.int/dev11/l-m/en#/http://id.who.int/icd/entity/849253504 )
Inclusion
fibromyalgia
fibromyositis
primary fibromyalgia syndrome LS18.00
( ICD-11's Descriptive text and Criteria for "Fibromyalgia Syndrome" is here:
https://icd.who.int/dev11/f/en#http://id.who.int/icd/entity/236601102 )
Coding hint
For coding the problem level, consider Pain functions 2F84
Index terms
CWP
primary fibromyalgia
ICPC-1
L18
ICPC-2
L18
ICD10
no exact corresponding class 00
Pain, not elsewhere classified R52
ICD11
Chronic widespread pain MG30.01
SNOMED CT
no exact corresponding term Id 00
chronic primary generalized pain (finding) Id 762590006
fibromyositis (disorder) Id 24693007
primary fibromyalgia syndrome (disorder) Id 95417003
Fibromyalgia is also coded in ICPC-3 as an inclusion under Chronic widespread pain.
There is also a sub code for
LS18.00 primary fibromyalgia syndrome
https://browser.icpc-3.info/index.php
LS Symptoms, complaints and abnormal findings of musculoskeletal system
LS18 Chronic widespread pain
Description
Chronic widespread pain (CWP) is diffuse pain in at least 4 of 5 body regions and is associated with significant emotional distress (anxiety, anger/frustration or depressed mood) and functional disability (interference in daily life activities and reduced participation in social roles). CWP is multifactorial: biological, psychological and social factors contribute to the pain syndrome. The diagnosis is appropriate when the pain is not directly attributable to a nociceptive process in those regions and there are features consistent with nociplastic pain and identified psychological and social contributors. Other chronic pain diagnoses to be considered are chronic cancer pain, chronic postsurgical or posttraumatic pain, chronic neuropathic pain, chronic visceral pain and chronic musculoskeletal pain.
( ICD-11's Description text and Criteria for Chronic widespread pain is here: https://icd.who.int/dev11/l-m/en#/http://id.who.int/icd/entity/849253504 )
Inclusion
fibromyalgia
fibromyositis
primary fibromyalgia syndrome LS18.00
( ICD-11's Descriptive text and Criteria for "Fibromyalgia Syndrome" is here:
https://icd.who.int/dev11/f/en#http://id.who.int/icd/entity/236601102 )
Coding hint
For coding the problem level, consider Pain functions 2F84
Index terms
CWP
primary fibromyalgia
ICPC-1
L18
ICPC-2
L18
ICD10
no exact corresponding class 00
Pain, not elsewhere classified R52
ICD11
Chronic widespread pain MG30.01
SNOMED CT
no exact corresponding term Id 00
chronic primary generalized pain (finding) Id 762590006
fibromyositis (disorder) Id 24693007
primary fibromyalgia syndrome (disorder) Id 95417003
Last edited:
DigitalDrifter
Senior Member (Voting Rights)
@Dx Revision Watch - Where is SEID (Systemic Exertion Intolerance Disease)?
Dx Revision Watch
Senior Member (Voting Rights)
@Dx Revision Watch - Where is SEID (Systemic Exertion Intolerance Disease)?
The term "Systemic Exertion Intolerance Disease (SEID)" has not been added to any of the following classification and terminology systems:
The U.S.'s ICD-10-CM.
Canada's ICD-10-CA.
Australia's ICD-10-AM.
Germany's ICD-10-GM.
The WHO's final release of ICD-10 (Version: 2019).
The WHO's forthcoming ICD-11.
SNOMED CT International Edition.
The various SNOMED CT national editions.
ICPC-2.
The forthcoming ICPC-3.
In November 2019, there was a proposal submitted via NHS Digital, who are responsible for maintenance of the SNOMED CT UK Edition, for addition of the term "Systemic Exertion Intolerance Disease" as a Synonym term under SNOMED CT Concept: 52702003 Chronic fatigue syndrome [1].
The request appeared to originate from an individual within the NHS, or other authorized user (possibly an NHS coder), as no other class of stakeholder was referenced as the original source of the request.
The request was referred for consideration to SNOMED International's terminology team who agreed that since the term has not been added to the U.S.'s ICD-10-CM by NCHS/CDC or adopted by any of the sponsor agencies of the IOM Panel's Report, it would be premature to add the term to SNOMED CT's International Edition [2].
References:
1 NHS Digital Request Submission Portal, SNOMED CT Submission Portal, Request #30104: https://isd.hscic.gov.uk/rsp-snomed/user/guest/request/view.jsf?request_id=30104
2 Update to report: NHS Digital requests addition of SEID to SNOMED CT v2 SNOMED CT Report Two | September 2020:
https://dxrevisionwatch.files.wordp...requests-addition-of-seid-to-snomed-ct-v2.pdf
Edited for clarity and to include links for SNOMED CT Submission Portal Request #30104 and my September 2020 update on the status of this request.
Last edited:
Dx Revision Watch
Senior Member (Voting Rights)
As I'm here, ATM, and had the following on file...
A virtual meeting of the U.S. National Committee on Vital and Health Statistics, Full Committee Meeting, took place on March 31-April 1, 2021:
Agenda: https://ncvhs.hhs.gov/meetings/full-committee-meeting-7/
On meeting Day One, there were two presentations on ICD-11 and the potential development of an ICD-11-CM adaptation for morbidity use:
An ICD-11 update from Margaret Skurka, NCVHS member:
Presentation slides: https://ncvhs.hhs.gov/wp-content/uploads/2021/04/H-ICD-Update-Margaret-Skurka-508.pdf
and
Comparative Analysis of ICD-10-CM with ICD-11 for Morbidity Coding from Kin-Wah Fung, Scientist, NIH/NLM:
Presentation slides: https://ncvhs.hhs.gov/wp-content/uploads/2021/04/I-ICD-Kin-Wah-508.pdf
which presented data drawn from this 2020 paper:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7309235/
The new International Classification of Diseases 11th edition: a comparative analysis with ICD-10 and ICD-10-CM
Kin Wah Fung, Julia Xu, and Olivier Bodenreider
Journal of the American Medical Informatics Association, 27(5), 2020, 738–746
doi: 10.1093/jamia/ocaa030
Slide #1:
Slide #32:
Slide #33:
Transcript of Meeting Day One: https://ncvhs.hhs.gov/wp-content/up...Full-Committee-Meeting-March-31-2021R-508.pdf
(The transcript for Margaret Skurka and Kin-Wah Fung's presentations starts on Page 66-75 of this transcript.)
The next NCVHS Full Committee Meeting is scheduled for September 9-10, 2021.
NCVHS has initiated the process of planning for transition to ICD-11 at the federal level. In November 2019, NCVHS sent a 7 page letter plus attachments to the HHS Secretary advising a research agenda and communications plan towards the adoption of ICD-11 for mortality use and the potential adaptation of ICD-11 for morbidity use [1]. NCVHS is looking into updating this letter.
1 November 25, 2019 The Honorable Alex Azar II Secretary Department of Health and Human Re: Preparing for Adoption of ICD-11 as a Mandated U.S. Health Data Standard:
https://ncvhs.hhs.gov/wp-content/up...-a-Mandated-US-Health-Data-Standard-final.pdf
A virtual meeting of the U.S. National Committee on Vital and Health Statistics, Full Committee Meeting, took place on March 31-April 1, 2021:
Agenda: https://ncvhs.hhs.gov/meetings/full-committee-meeting-7/
On meeting Day One, there were two presentations on ICD-11 and the potential development of an ICD-11-CM adaptation for morbidity use:
An ICD-11 update from Margaret Skurka, NCVHS member:
Presentation slides: https://ncvhs.hhs.gov/wp-content/uploads/2021/04/H-ICD-Update-Margaret-Skurka-508.pdf
and
Comparative Analysis of ICD-10-CM with ICD-11 for Morbidity Coding from Kin-Wah Fung, Scientist, NIH/NLM:
Presentation slides: https://ncvhs.hhs.gov/wp-content/uploads/2021/04/I-ICD-Kin-Wah-508.pdf
which presented data drawn from this 2020 paper:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7309235/
The new International Classification of Diseases 11th edition: a comparative analysis with ICD-10 and ICD-10-CM
Kin Wah Fung, Julia Xu, and Olivier Bodenreider
Journal of the American Medical Informatics Association, 27(5), 2020, 738–746
doi: 10.1093/jamia/ocaa030
Slide #1:
Slide #32:
Slide #33:
Transcript of Meeting Day One: https://ncvhs.hhs.gov/wp-content/up...Full-Committee-Meeting-March-31-2021R-508.pdf
(The transcript for Margaret Skurka and Kin-Wah Fung's presentations starts on Page 66-75 of this transcript.)
The next NCVHS Full Committee Meeting is scheduled for September 9-10, 2021.
NCVHS has initiated the process of planning for transition to ICD-11 at the federal level. In November 2019, NCVHS sent a 7 page letter plus attachments to the HHS Secretary advising a research agenda and communications plan towards the adoption of ICD-11 for mortality use and the potential adaptation of ICD-11 for morbidity use [1]. NCVHS is looking into updating this letter.
1 November 25, 2019 The Honorable Alex Azar II Secretary Department of Health and Human Re: Preparing for Adoption of ICD-11 as a Mandated U.S. Health Data Standard:
https://ncvhs.hhs.gov/wp-content/up...-a-Mandated-US-Health-Data-Standard-final.pdf
Dx Revision Watch
Senior Member (Voting Rights)
Please see my note at the end of this post.
--------------------------------------------------
https://solvecfs.org/solve-m-e-and-...phic-lack-of-me-cfs-case-tracking-in-the-u-s/
SOLVE M.E. AND SIX OTHER ORGANIZATIONS TACKLE CATASTROPHIC LACK OF ME/CFS CASE TRACKING IN THE U.S.
AUGUST 23, 2021 / KARMAN KREGLOE / ADVOCACY, LONG COVID AND POST INFECTION DISEASES, NEWS, PRESENTATIONS, CONFERENCES, & WEBINARS
Together with six other organizations, we have submitted a proposal to the National Center for Health Statistics (NCHS) to add myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) to the neurological chapter of the International Classification of Diseases (ICD-10-CM).
Read our press release here.
Today, ME/CFS does not exist in the US ICD-10-CM. Instead, most US doctors assign the code for chronic fatigue syndrome which has the same code as the symptom of chronic fatigue. As a result, it is impossible to accurately track the mortality and morbidity of ME/CFS or its relationship to Long Covid. This affects not only the 836,000 to 2.5 million Americans with ME/CFS but also the tsunami of Long Covid patients who could develop ME/CFS.
Our partners in this proposal include the International Association for Chronic Fatigue Syndrome/Myalgic Encephalomyelitis, #MEAction, Open Medicine Foundation, Massachusetts ME/CFS & FM Association, the Minnesota ME/CFS Alliance, and Pandora Org. This proposal will be discussed at the upcoming meeting of the NCHS ICD-10-CM Maintenance Committee on September 14-15, 2021. Details on registration and the time slot for this proposal will be provided when available.
--------------------------------------------------------------------------------------
Please note that I have had no involvement in this submission.
My opinion:
The term currently listed in ICD-10-CM as the inclusion term under G93.3 Postviral fatigue syndrome is "Benign myalgic encephalomyelitis".
A request for deleting the prefix "Benign", bringing ICD-10-CM in line with the deletion of the prefix "Benign" that was implemented for the final update of the WHO's ICD-10 (Version: 2019, released January 2020) and in line with ICD-11 (Version: 05/2021) would also need to be submitted for.
If a sub-code is requested to be assigned to existing term "[Benign] myalgic encephalomyelitis" and the conjoined terms and conjoined acronyms:
"myalgic encephalomyelitis/chronic fatigue syndrome"
"ME/CFS"
are proposed to be added as inclusions under new sub-code: "Myalgic encephalomyelitis", I think it likely that NCHS and CDC's response would be that conjoined terms would present data aggregation/disaggregation problems (backward and going forwards) for both the US and for WHO international statistical analysis and that the terms would need to be included as separate 5 character sub-codes under a 4 character code, for example:
G93.3 Postviral and related fatigue syndromes
G93.30 Postviral fatigue syndrome
G93.31 Myalgic encephalomyelitis
Index Term
ME - [Myalgic encephalomyelitis] (The format the WHO is using for acronyms for ICD-11)*
G93.32 Chronic fatigue syndrome
Chronic fatigue syndrome NOS
Index Term
CFS - [Chronic fatigue syndrome]
or
G93.3 Postviral and related fatigue syndromes
G93.30 Postviral fatigue syndrome
G93.31 Myalgic encephalomyelitis
Chronic fatigue syndrome
Index Terms
ME - [Myalgic encephalomyelitis]
CFS - [Chronic fatigue syndrome]
Edited to add: Though I think the first of these hypothetical hierarchies would be more likely acceptable to NCHS/CDC, ie. with a unique sub-code assigned to Chronic fatigue syndrome, rather than coded as an inclusion under Myalgic encephalomyelitis.
Edited to add: For ICD-11, the following acronyms, with the term in full appearing in square brackets, have been listed under Index Terms to 8E49 Postviral fatigue syndrome. Note this is the standard format for listing acronyms in ICD-11.
https://icd.who.int/dev11/l-m/en#/http://id.who.int/icd/entity/569175314
Note also that the text states: "The most recent version is ICD-11 but most countries use ICD-10."
The earliest ICD-11 can be implemented by member states is from January 01, 2022, as the WHA's endorsement of ICD-11 does not come into effect until that date. Most member states won't be ready to migrate from ICD-10 (or from a clinical modification of ICD-10) for several years.
The text mentions "SEID". I would not support the addition of the term "Systemic exertion intolerance disease" or "SEID - [Systemic Exertion Intolerance Disease]" or both to either ICD-11, ICD-10-CM, SNOMED-CT International Edition, or any of the national editions of SNOMED-CT.
--------------------------------------------------
https://solvecfs.org/solve-m-e-and-...phic-lack-of-me-cfs-case-tracking-in-the-u-s/
SOLVE M.E. AND SIX OTHER ORGANIZATIONS TACKLE CATASTROPHIC LACK OF ME/CFS CASE TRACKING IN THE U.S.
AUGUST 23, 2021 / KARMAN KREGLOE / ADVOCACY, LONG COVID AND POST INFECTION DISEASES, NEWS, PRESENTATIONS, CONFERENCES, & WEBINARS
Together with six other organizations, we have submitted a proposal to the National Center for Health Statistics (NCHS) to add myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) to the neurological chapter of the International Classification of Diseases (ICD-10-CM).
Read our press release here.
Today, ME/CFS does not exist in the US ICD-10-CM. Instead, most US doctors assign the code for chronic fatigue syndrome which has the same code as the symptom of chronic fatigue. As a result, it is impossible to accurately track the mortality and morbidity of ME/CFS or its relationship to Long Covid. This affects not only the 836,000 to 2.5 million Americans with ME/CFS but also the tsunami of Long Covid patients who could develop ME/CFS.
Our partners in this proposal include the International Association for Chronic Fatigue Syndrome/Myalgic Encephalomyelitis, #MEAction, Open Medicine Foundation, Massachusetts ME/CFS & FM Association, the Minnesota ME/CFS Alliance, and Pandora Org. This proposal will be discussed at the upcoming meeting of the NCHS ICD-10-CM Maintenance Committee on September 14-15, 2021. Details on registration and the time slot for this proposal will be provided when available.
We will be holding a webinar and listening session on September 2 at 10 AM PT / 1 PM ET to discuss the proposal and hear any concerns and answer questions. You can register in advance for this meeting at this link.
Details
The World Health Organization publishes a standardized system called the International Classification of Diseases (ICD) to track diseases globally. The most recent version is ICD-11 but most countries use ICD-10. Both the ICD-10 and the ICD-11 classify ME and CFS in the neurological chapter under the lead term of “postviral fatigue syndrome.”
The US version of the ICD-10 is the ICD-10-CM and is used to code diseases in medical records. When ICD-10-CM was implemented in 2015, CFS was moved from the neurological chapter to the Signs and Symptoms chapter and given the same code as the symptom of “chronic fatigue, unspecified.” The term ME/CFS was never added so US doctors must choose either CFS or ME. They almost always choose CFS.
As a result, virtually all cases of ME/CFS in medical records have been dumped into the “chronic fatigue, unspecified” bucket. Using the same code for both ME/CFS and the symptom of “chronic fatigue, unspecified” makes it impossible to track the mortality and morbidity of ME/CFS separate from the symptom of nonspecific chronic fatigue. This impacts insurance reimbursement, generation of statistics on disease burden and outcomes, the medical perception of ME/CFS. And it makes it virtually impossible to identify ME/CFS cases in retrospective research using electronic health records, such as that being done for Long COVID.
The submitted proposal recommends the following three changes to ICD-10-CM to address this problem:
The submitted proposal did not make recommendations regarding the term “chronic fatigue syndrome” because of the lack of consensus on earlier proposals on how this should be addressed.
- Expand the lead term, “postviral fatigue syndrome,” to “postviral and related fatigue syndromes” to allow for non-viral triggers. ICD rules limit options for the new name as it needs to include the original name
- Add separate subcodes for postviral fatigue syndrome and ME
- Add the terms “myalgic encephalomyelitis/chronic fatigue syndrome” and “ME/CFS” as inclusions of ME
For more information, see the FAQs at this link.
https://docs.google.com/document/d/1kyHuHXPZ0nxzF2jIZelyeZqiuq0KWfmm/edit
Proposal to add ME/CFS to the ICD-10-CM August 23, 2021
Frequently Asked Questions
Background:
Seven ME/CFS organizations have submitted a proposal to the National Center for Health Statistics (NCHS) to add myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) to the neurological chapter of the International Classification of Diseases (ICD-10-CM).
Today, ME/CFS does not exist in the US ICD-10-CM. Instead, most US doctors assign the code for chronic fatigue syndrome which has the same code as the symptom of chronic fatigue. As a result, it is impossible to accurately track the mortality and morbidity of ME/CFS or its relationship to Long COVID. This affects not only the 836,000 to 2.5 million Americans with ME/CFS but also the tsunami of Long COVID patients who could develop ME/CFS.
The organizations submitting this proposal include the International Association for Chronic Fatigue Syndrome/Myalgic Encephalomyelitis, #MEAction, Open Medicine Foundation, Solve M.E., Massachusetts ME/CFS & FM Association, the Minnesota ME/CFS Alliance, and Pandora Org.
This proposal will be discussed at the upcoming meeting of the NCHS ICD-10-CM Maintenance Committee on September 14-15, 2021. Details on the exact time and date of that meeting will be provided when they are available.
ICD stands for the International Classification of Diseases and is produced by the World Health Organization. It is used to track the mortality and morbidity of diseases globally. WHO has recently released ICD-11 but most countries are using ICD-10, published in 1990 and will likely do so for a number of years.
- What is the ICD-10-CM and why is it used?
Countries are allowed to produce their own clinical modifications as long as they follow WHO standards. The US version of the ICD-10 is the ICD-10-CM, released in 2015. The ICD-10-CM is used in electronic health records to code the diagnoses provided by doctors.
The term “ME/CFS” does not exist in the ICD-10 or ICD-10-CM, even though the US federal agencies and numerous medical education providers have adopted the term. The only terms that exist are “ME” and “CFS.”
- How is ME/CFS classified in the ICD-10 and the ICD-10-CM?
The WHO classifies ME and CFS in the neurological chapter of both ICD-10 and ICD-11 under the lead term “postviral fatigue syndrome (PVFS).” The US also classifies ME in the neurological chapter of ICD-10-CM under PVFS. However, when the ICD-10-CM was rolled out in the US in 2015, the US relocated CFS to the Symptoms chapter and gave it the same code as the symptom of “chronic fatigue.” The US is the only country in the world to have done this. This is not aligned with either ICD-10 or ICD-11.
Attendees at a previous meeting on ICD-10-CM held by the National Center for Health Statistics (NCHS), the CDC group that manages ICD-10-CM, stated that ME is seldom seen in medical records. The vast majority of US doctors use the term “CFS.” And if a doctor were to record a diagnosis of ME/CFS, the person assigning the code in the medical record would have to choose either the code for CFS or for ME since there is no code for ME/CFS. As a result, the vast majority of Americans diagnosed with ME/CFS in the US will end up with the code for the symptom of “chronic fatigue, unspecified” in their medical records instead.
This makes it impossible to track and report on the mortality and morbidity of cases of ME/CFS separate from the symptom of non-specific chronic fatigue due to any cause. This likely impedes insurance reimbursement, generation of statistics on disease burden and outcomes, the medical perception of ME/CFS. And it also makes it virtually impossible to identify ME/CFS cases in retrospective research using electronic health records, such as that being done for Long COVID.
- What difference does the lack of an ICD-10-CM code for ME/CFS make?
Before the pandemic, this affected an estimated 1 to 2.5 million Americans with ME/CFS, leaving them effectively lost in the medical system.
- Who does this affect?
These numbers are expected to grow significantly, given the risk of people developing ME/CFS following an acute COVID-19 infection. While no firm estimates exist, previous studies suggest that as many as 10-12% of people can develop ME/CFS following an infection. This could translate to millions of new cases of ME/CFS. Some Long COVID patients, those experiencing prolonged symptoms post-COVID, have already been diagnosed with ME/CFS. And emerging clinical care guidance for Long COVID is already recognizing the potential link.
Proposals were submitted to NCHS in 2011, 2012 and again in 2017 to move CFS back to the neurological chapter. But these proposals were rejected because of lack of stakeholder consensus on how to resolve this problem. Stakeholders to the NCHS process include groups such as the medical community, the patient community, and hospital and coding associations.
- Why has this problem not been addressed before?
Examples of areas of lack of consensus included:
Note that WHO has said terms should not be moved from one place to another unless robust science supports that decision. This is in part why ME and CFS remain in the neurological chapter in ICD-11, since it was located there in ICD-10.
- Whether or not CFS should be moved back to the neurological chapter at all since it has been used as a wastebin diagnosis and/or because it has not been proven to be specifically neurological.
- Whether CFS and ME are the same thing and should have the same code or are different and need different codes. Whether doctors will be confused if CFS and ME have different codes
- Whether CFS belongs under postviral fatigue syndrome since it is not always postviral
- Whether SEID should be added (discussed in the 2017 meeting but the term has not been adopted)
In December 2020, seven organizations, listed below, submitted a proposal to NCHS asking for three primary changes:
- What is being proposed now to address the lack of an ICD-10-CM code for ME/CFS?
- Change the lead term from “postviral fatigue syndrome” to “postviral and other related fatigue syndromes” because ME can be triggered by both viral and non-viral causes
- Note that WHO rules require that the words in the current title, “postviral fatigue syndrome,” are also in the new title so options for this lead term are limited.
- Establish different codes for ME and PVFS since PVFS is always postviral and ME can be triggered by other causes. ME/CFS will use the same code as ME.
- Add the terms “myalgic encephalomyelitis/chronic fatigue syndrome” and “ME/CFS” as “inclusion” terms (essentially synonyms) of the term “myalgic encephalomyelitis”
The submitted proposal focused on getting the term ME/CFS added as doctors are using that term and it needs to be in the ICD-10-CM. It dd not ask to have the term “chronic fatigue syndrome” moved to the neurological chapter because stakeholders rejected the various proposals for resolving this in the last three proposals.
The seven organizations that submitted the proposal to NCHS are:
The International Association for Chronic Fatigue Syndrome/Myalgic Encephalomyelitis, #MEAction, Open Medicine Foundation, Solve M.E., Massachusetts ME/CFS & FM Association, Minnesota ME/CFS Alliance, and Pandora Org,
This proposal is scheduled to be discussed at the ICD-10-CM Coordination and Maintenance Committee meeting on September 14-15, 2021. After the meeting, there will be an opportunity for public comment prior to a final decision by NCHS. If the proposal is accepted, the change would be implemented in October 2022.
- When will this change to ICD-10-CM be implemented if it is approved?
No, this does not fully address the problem...
- Does this resolve the problem? If no, why not and what else needs to be done?
First, the proposal submitted by the organizations does not address how CFS is classified in the US ICD-10-CM.
Second, ME/CFS patients who currently have a CFS diagnosis will have to have the new code added to their medical record in order for them to be properly tracked. If not done, they will continue to be subsumed under the symptom of “chronic fatigue, unspecified” in medical records.
Some people with Long COVID may develop and be diagnosed with ME/CFS. This will ensure they are correctly tracked and not dumped into the “chronic fatigue, unspecified” bucket.
- Does this impact people with Long COVID?
It is difficult to get disability for ME/CFS in the US. But this change should not impact that. The 2014 Social Security Administration (SSA) ruling for this disease used the term “CFS” but referenced the 2003 ME/CFS Canadian Consensus Criteria and the 2011 ME International Consensus Criteria. Since then, SSA has published the 2018 guide for healthcare professionals that refers to the disease as Myalgic Encephalomyelitis/Chronic Fatigue Syndrome.
- Does this affect the ability of people with ME/CFS to get disability?
[Ends]
--------------------------------------------------------------------------------------
Please note that I have had no involvement in this submission.
My opinion:
The term currently listed in ICD-10-CM as the inclusion term under G93.3 Postviral fatigue syndrome is "Benign myalgic encephalomyelitis".
A request for deleting the prefix "Benign", bringing ICD-10-CM in line with the deletion of the prefix "Benign" that was implemented for the final update of the WHO's ICD-10 (Version: 2019, released January 2020) and in line with ICD-11 (Version: 05/2021) would also need to be submitted for.
If a sub-code is requested to be assigned to existing term "[Benign] myalgic encephalomyelitis" and the conjoined terms and conjoined acronyms:
"myalgic encephalomyelitis/chronic fatigue syndrome"
"ME/CFS"
are proposed to be added as inclusions under new sub-code: "Myalgic encephalomyelitis", I think it likely that NCHS and CDC's response would be that conjoined terms would present data aggregation/disaggregation problems (backward and going forwards) for both the US and for WHO international statistical analysis and that the terms would need to be included as separate 5 character sub-codes under a 4 character code, for example:
G93.3 Postviral and related fatigue syndromes
G93.30 Postviral fatigue syndrome
G93.31 Myalgic encephalomyelitis
Index Term
ME - [Myalgic encephalomyelitis] (The format the WHO is using for acronyms for ICD-11)*
G93.32 Chronic fatigue syndrome
Chronic fatigue syndrome NOS
Index Term
CFS - [Chronic fatigue syndrome]
or
G93.3 Postviral and related fatigue syndromes
G93.30 Postviral fatigue syndrome
G93.31 Myalgic encephalomyelitis
Chronic fatigue syndrome
Index Terms
ME - [Myalgic encephalomyelitis]
CFS - [Chronic fatigue syndrome]
Edited to add: Though I think the first of these hypothetical hierarchies would be more likely acceptable to NCHS/CDC, ie. with a unique sub-code assigned to Chronic fatigue syndrome, rather than coded as an inclusion under Myalgic encephalomyelitis.
Edited to add: For ICD-11, the following acronyms, with the term in full appearing in square brackets, have been listed under Index Terms to 8E49 Postviral fatigue syndrome. Note this is the standard format for listing acronyms in ICD-11.
https://icd.who.int/dev11/l-m/en#/http://id.who.int/icd/entity/569175314
- CFS - [chronic fatigue syndrome]
- ME - [myalgic encephalomyelitis]
- PVFS - [postviral fatigue syndrome]
Note also that the text states: "The most recent version is ICD-11 but most countries use ICD-10."
The earliest ICD-11 can be implemented by member states is from January 01, 2022, as the WHA's endorsement of ICD-11 does not come into effect until that date. Most member states won't be ready to migrate from ICD-10 (or from a clinical modification of ICD-10) for several years.
The text mentions "SEID". I would not support the addition of the term "Systemic exertion intolerance disease" or "SEID - [Systemic Exertion Intolerance Disease]" or both to either ICD-11, ICD-10-CM, SNOMED-CT International Edition, or any of the national editions of SNOMED-CT.
Last edited by a moderator:
Thank you for posting, Susie.
The proposal submitted by the seven organizations does not include a recommendation to add the term SEID.
The submitted proposal does request the removal of the word "benign" from the term "myalgic encephalomyelitis," the revision of exclusions as needed to reflect the changes (e.g. removal of "benign"), and the addition of an exclusion for neurasthenia on the G93.3 term. I've updated the FAQ to include these smaller requests.
The proposal submitted by the seven organizations does not include a recommendation to add the term SEID.
The submitted proposal does request the removal of the word "benign" from the term "myalgic encephalomyelitis," the revision of exclusions as needed to reflect the changes (e.g. removal of "benign"), and the addition of an exclusion for neurasthenia on the G93.3 term. I've updated the FAQ to include these smaller requests.
Dx Revision Watch
Senior Member (Voting Rights)
Thank you for posting, Susie.
The proposal submitted by the seven organizations does not include a recommendation to add the term SEID.
Yes. I've said in my notes that: The text mentions "SEID" - not that the proposals include a recommendation to add the term SEID. I have highlighted the mention of "SEID" in the text as I wish to make my own position on "SEID" clear.
The submitted proposal does request the removal of the word "benign" from the term "myalgic encephalomyelitis," the revision of exclusions as needed to reflect the changes (e.g. removal of "benign"), and the addition of an exclusion for neurasthenia on the G93.3 term. I've updated the FAQ to include these smaller requests.
I may have missed it somewhere in the materials accompanying this press release but when the prefix "Benign" was deleted from the Tabular List inclusion term, "Benign myalgic encephalomyelitis" for the final update of the WHO's International version of ICD-10 (Version: 2019, published January 2020), the legacy term "Benign myalgic encephalomyelitis" was retained as an Index term.
Likewise for ICD-11, when the deletion of the prefix "Benign" was implemented, in November 2020, the legacy term "Benign myalgic encephalomyelitis" was retained, as requested, as an Index term, in order that legacy data collected using the former term can be carried forward.
It is likely that NCHS/CDC would also want to retain a listing for the legacy term in the ICD-10-CM Alphabetical Index.
The ICD-10-CM legacy classification is for two unique coded-for ICD terms:
[Benign] myalgic encephalomyelitis (for ICD-10-CM, currently an inclusion under G93.3)
Chronic fatigue syndrome (for ICD-10-CM, as "Chronic fatigue syndrome NOS*", currently an inclusion under R53.82)
*NOS = "Not otherwise specified". This abbreviation is the equivalent of unspecified.
If the proposed restructuring assigns a new five character sub-code, for example, G93.31 to Myalgic encephalomyelitis, I consider it would be contra to WHO ICD-10 conventions to list the conjoined term
"myalgic encephalomyelitis/chronic fatigue syndrome"
(a term that is not included in any WHO ICD edition) as an inclusion term under that new sub-code, for example, as:
G93.31 Myalgic encephalomyelitis
Myalgic encephalomyelitis/chronic fatigue syndrome
ME/CFS
since that would combine two historically discrete (or mutually exclusive) ICD entities to form a new ICD entity. (The conjoined acronyms, "ME/CFS", would not in any case be acceptable format for a Tabular List inclusion term.)
For previous submissions to the ICD-10-CM Coordination and Maintenance Committee, it has often been the case that Donna Pickett has proffered an alternative structure which is included on the agenda for discussion alongside the submitted proposals, or has suggested revisions to the proposed submission before accepting it for tabling on the agenda.
I do not recall any alternative structure being proposed by Ms Pickett which has recommended joining "myalgic encephalomyelitis" and "chronic fatigue syndrome" together and listing these existing discrete ICD entity terms as a conjoined term, either assigned to a new sub-code or as an inclusion under a new sub-code.
I am surprised that the various groups involved with this submission have not given consideration to WHO ICD-10 taxonomic principles and conventions, in the specific context of the WHO's requirements for analysis of legacy data and future data collection.
Last edited: