Partial transcript from the last 5 minutes of the circa 20 minute presentation:
Agenda topic:
Page 167: Postural orthostatic tachycardia syndrome (POTS)
[Note: This extract discussing use of acronyms in ICD-10-CM is a cleaned up transcript based on the automatic audio transcript. I've striven for accuracy but some transcribing errors may remain.]
David Berglund
05:17:51 Thank you Lauren Styles. And next, let's move to the coding; this is on page 168 for those following along.
Looking at the Tabular modifications that are being proposed here at
G90 Disorders of autonomic nervous system, it's being proposed to add a new code G90.A for Postural orthostatic tachycardia syndrome, with also inclusion terms to be added as Chronic orthostatic intolerance and Postural tachycardia syndrome. So that's a fairly brief set of changes being proposed. Do we have any comments questions or other things here? It looks like Dr Remer is raising hand.
Erica Remer
05:18:45 Yeah, we need to stick "POTS" in there, too, don't you think, for the inclusion?
David Berglund
05:18:52 You'd like to see just "POTS", yeah, P...O...T...S?
Erica Remer
05:18:55 Yes, thanks.
David Berglund
05:18:59 Not to be confused with Cause of injury: "Getting hit with a pot" or something?
Jeff Boris
05:19:05 More importantly, not to be confused with Pot's, "P...O...T...S" -
Pot's disease, which is spinal tuberculosis and I can't tell you the number of times that I have seen that and it's an incorrect diagnosis for these patients.
Erica Remer
05:19:22 That would be quite a surprise to them: Oh, I have tuberculosis.
Jeff Boris
Correct. That's an old eponym.
David Berglund
05:19:32 Yeah, yeah, that's a good question too, then. So that is one we can look at; we don't always include all of the potential abbreviations that can be found, but that is one we can at least look further at.
I think there were some concerns internally, that the term "POTS" might be confusing for some people, and certainly the "Pot's spinal tuberculosis that may be one that we have indexed, I suppose, that's well - an older term - as it were, that could get confusing if people...
Erica Remer
05:20:16 I think you should take a look at your explanation up above on Page 167 - use "POTS" all over the place.
05:20:25 And I think you know as a clinician, I used to use "POTS" all the time, so I would think that you know, like you, don't want the coders to have to go query a doctor, did you really mean "Postural orthostatic tachycardia syndrome" if they use the acronym "POTS", just saying.
David Berglund
05:20:42 I remember, I remember as an intern, getting quizzed on using the term "COPD", my goodness.
Erica Remer
05:20:52 You are showing your age, David.
[Laughter]
David Berglund
05:20:57 Yeah, yeah, oh goodness.
Jeff Boris
05:21:00 And actually, David, just in case you really want to get particular, there is another use of the term "POTTS" - P...O...T...T...S, so two "Ts - which is a left subclavian to, to... pulmonary shunt, that used to be used prior to the Blalock–Taussig-Thomas shunt - patients who have cyanotic congenital cardiac disease.
David Berglund
05:21:29 So if some of these do get a little confusing, I suppose, that is, I will definitely acknowledge, one reason we sometimes get a little hesitant about adding abbreviations to ICD, itself; we will take this under advisement and we could at least consider using the four letters "POTS" to refer to this; although, given the potential for other types of use or meaning, we tend to encourage people to spell it out if they can, but that said, well it's enough words that are long enough that I can see how people don't always want to do that.
David Berglund
05:22:21 All right, other...
We have a comment from Penelope Deotte?
Penelope Deotte
05:22:29 Yes, Penelope Deotte from Optum360 and my only other comment was - we do have the convention, where we could put the acronym in the code title in brackets, we have that in a few places and [barely audible: rather than?] an inclusion term...we could do that. But I'll put that in my comments as just another thought.
David Berglund
05:22:57 And that is something we will contemplate. I won't give any final decisions on that aspect but we'll be considering this and we appreciate comments in writing by email on this, we'll be glad to look at that.
Any other comments or questions at this time?
Marvelyn Davis [Moderator]
05:23:22 Not at this time.
David Berglund
05:23:25 All right.
Thank you, thank you, Dr Boris for presenting.
Jeff Boris
05:23:31 Thank you for this opportunity, appreciate it.
[Discussion of topic item ends]
---------------------------------------------------------------------------
Note that the term:
Postural orthostatic tachycardia syndrome has been included in ICD-11 since at least 2016 and is discretely coded for in both the ICD-11 Foundation (the linearization that contains all the entities) and the ICD-11 MMS (the ICD-11 equivalent to the Tabular List which contains a sub-linearization of the Foundation).
https://icd.who.int/dev11/f/en#/http://id.who.int/icd/entity/1533647472
https://icd.who.int/dev11/l-m/en#/http://id.who.int/icd/entity/1533647472
8D89.2 Postural orthostatic tachycardia syndrome
Note also: The acronym "POTS" has not been included under Synonyms/All Index Terms (nor has it been added to the end of the concept title term in brackets). Nor is the acronym "POTS" included in the data base for the ICD-11 Coding Tool (which functions as ICD-11's electronic Index).
I would suggest that a POTS advocacy org and/or clinical allies request the addition, via the Proposal Mechanism, of the acronym:
POTS - [postural orthostatic tachycardia syndrome]
under
All Index Terms.
For ICD-11, the convention for acronyms is:
An acronym is an abbreviation formed from the first letters of other words and pronounced as a word (e.g. NASA). Acronyms may never be used for titles of categories. They should be added as synonyms to the appropriate spelt out disease entity thus facilitating identification of the relevant cases and categories.
The ICD-11 convention format is, for example:
Under
Synonyms/
All Index Terms:
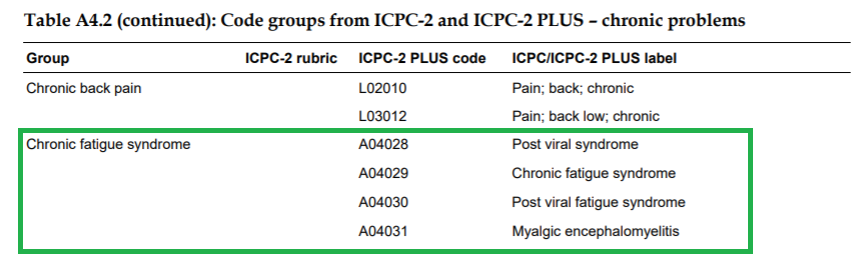
- CFS - [chronic fatigue syndrome]
- ME - [myalgic encephalomyelitis]
- PVFS - [postviral fatigue syndrome]