Dx Revision Watch
Senior Member (Voting Rights)
Resurfacing briefly from retirement to clarify and update on the following extract from the IAFME document:
On Page 6, the document states (my highlighting):
1 For clarity: Benign myalgic encephalomyelitis was included in the Index, only, for the WHO's ICD-8 and ICD-9. It was not included in both the Index and the Tabular List until ICD-10 was published in 1992.
Reference and screenshots from ICD-8 and ICD-9: Post #172: https://www.s4me.info/threads/who-w...-leads-to-poor-outcome.5109/page-9#post-96715
2 Dr Tarun Dua is a medical officer working on the Program for Neurological Diseases and Neuroscience, Management of Mental and Brain Disorders, WHO Department of Mental Health and Substance Abuse. This WHO department has responsibility for both mental disorders and neurological diseases and disorders. Its Director is Dr Shekhar Saxena.
Dr Dua had acted as lead WHO Secretariat and Managing Editor for ICD Revision’s Topic Advisory Group (TAG) for Neurology, an external working group chaired by Prof Raad Shakir. TAG Neurology was sunsetted in October 2016.
The proposal submitted by Dr Tarun Dua (November 06, 2017) was stated by Dr Dua as "[having] been submitted on behalf of Topic Advisory Group (TAG) on Diseases of the Nervous System, and reiterates the TAG’s earlier conclusions.”
On November 19, 2018, the proposal submitted by Dua, in November 2017, was marked as Rejected by ICD-11 Proposal platform admins:
https://icd.who.int/dev11/proposals/f/en#/http://id.who.int/icd/entity/569175314
This decision to reject the Dua/TAG Neurology proposal recommending that the terms should be relocated under the Symptoms, signs chapter is accompanied by this brief rationale from ICD-11 Proposal Platform admins “Team3 WHO”:
Screenshot: Accessed November 22, 2018:

Importantly, the decision to retain the terms in the Disorders of the nervous system chapter is supported by the WHO MSAC and CSAC* committees.
*The Classifications and Statistics Advisory Committee (CSAC) takes over the role of the ICD-10 Update and Revision Committee (URC). The last update for ICD-10 will be 2019.
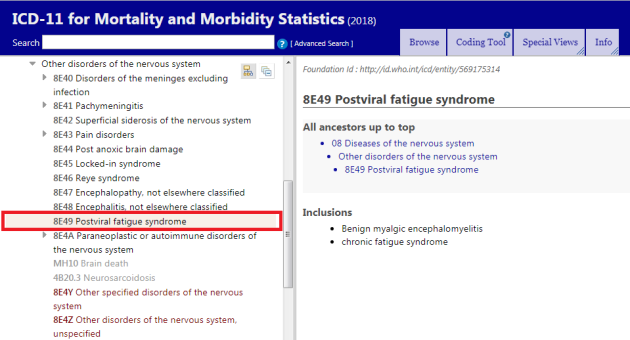
With the Dua/TAG Neurology proposal rejected by WHO classification experts and the MSAC and CSAC committees, this means that these ICD-10 legacy terms continue to stand as per the “Implementation” version of the ICD-11 MMS which was published in June 2018:
https://icd.who.int/browse11/l-m/en#/http://id.who.int/icd/entity/569175314
Action for ME were informed of this development on November 20.
My November 22 report on this development can be read at:
Update on the status of the classification of PVFS, ME and CFS for ICD-11: Part Three: WHO rejects Dr Dua’s proposal
https://dxrevisionwatch.com/2018/11...d-11-part-three-who-rejects-dr-duas-proposal/
On Page 6, the document states (my highlighting):
"Disease classification
"The World Health Organization (WHO) added ME to the neurological chapter of the International Classification of Diseases (ICD) in 1969. In the ICD-10, ME is an inclusion term under post-viral fatigue syndrome (code G93.3). Following two outbreaks in the mid-1980s, the US coined the alternative term “chronic fatigue syndrome,” which the WHO added to ICD-10 and indexed to “post-viral fatigue syndrome.” In its version of the ICD-10 (the ICD10-CM), the US reclassified CFS to be equivalent to the symptom of “chronic fatigue, unspecified” while leaving ME in the neurological chapter. In the ICD-11, the terms “ME” and “CFS” are in the neurological chapter following the precedent set in ICD-10. But WHO staff have submitted an ICD-11 proposal to reclassify the terms to the Signs and Symptoms chapter under the musculoskeletal system section based on the claim that there is no evidence of neurological impairment and that the disease is perpetuated by psychological processes (Dua, 2017). These claims are not supported by the evidence of neurological, immunological, and energy metabolism impairment. (National Academy of Medicine 2015; Komaroff & Cho, 2011; Komaroff et al, 2018a). The WHO has stated that no decision will be made on proposals to change the classification until they complete a systematic review..."
"The World Health Organization (WHO) added ME to the neurological chapter of the International Classification of Diseases (ICD) in 1969. In the ICD-10, ME is an inclusion term under post-viral fatigue syndrome (code G93.3). Following two outbreaks in the mid-1980s, the US coined the alternative term “chronic fatigue syndrome,” which the WHO added to ICD-10 and indexed to “post-viral fatigue syndrome.” In its version of the ICD-10 (the ICD10-CM), the US reclassified CFS to be equivalent to the symptom of “chronic fatigue, unspecified” while leaving ME in the neurological chapter. In the ICD-11, the terms “ME” and “CFS” are in the neurological chapter following the precedent set in ICD-10. But WHO staff have submitted an ICD-11 proposal to reclassify the terms to the Signs and Symptoms chapter under the musculoskeletal system section based on the claim that there is no evidence of neurological impairment and that the disease is perpetuated by psychological processes (Dua, 2017). These claims are not supported by the evidence of neurological, immunological, and energy metabolism impairment. (National Academy of Medicine 2015; Komaroff & Cho, 2011; Komaroff et al, 2018a). The WHO has stated that no decision will be made on proposals to change the classification until they complete a systematic review..."
1 For clarity: Benign myalgic encephalomyelitis was included in the Index, only, for the WHO's ICD-8 and ICD-9. It was not included in both the Index and the Tabular List until ICD-10 was published in 1992.
Reference and screenshots from ICD-8 and ICD-9: Post #172: https://www.s4me.info/threads/who-w...-leads-to-poor-outcome.5109/page-9#post-96715
2 Dr Tarun Dua is a medical officer working on the Program for Neurological Diseases and Neuroscience, Management of Mental and Brain Disorders, WHO Department of Mental Health and Substance Abuse. This WHO department has responsibility for both mental disorders and neurological diseases and disorders. Its Director is Dr Shekhar Saxena.
Dr Dua had acted as lead WHO Secretariat and Managing Editor for ICD Revision’s Topic Advisory Group (TAG) for Neurology, an external working group chaired by Prof Raad Shakir. TAG Neurology was sunsetted in October 2016.
The proposal submitted by Dr Tarun Dua (November 06, 2017) was stated by Dr Dua as "[having] been submitted on behalf of Topic Advisory Group (TAG) on Diseases of the Nervous System, and reiterates the TAG’s earlier conclusions.”
On November 19, 2018, the proposal submitted by Dua, in November 2017, was marked as Rejected by ICD-11 Proposal platform admins:
https://icd.who.int/dev11/proposals/f/en#/http://id.who.int/icd/entity/569175314
This decision to reject the Dua/TAG Neurology proposal recommending that the terms should be relocated under the Symptoms, signs chapter is accompanied by this brief rationale from ICD-11 Proposal Platform admins “Team3 WHO”:
Screenshot: Accessed November 22, 2018:
Importantly, the decision to retain the terms in the Disorders of the nervous system chapter is supported by the WHO MSAC and CSAC* committees.
*The Classifications and Statistics Advisory Committee (CSAC) takes over the role of the ICD-10 Update and Revision Committee (URC). The last update for ICD-10 will be 2019.
With the Dua/TAG Neurology proposal rejected by WHO classification experts and the MSAC and CSAC committees, this means that these ICD-10 legacy terms continue to stand as per the “Implementation” version of the ICD-11 MMS which was published in June 2018:
https://icd.who.int/browse11/l-m/en#/http://id.who.int/icd/entity/569175314
Action for ME were informed of this development on November 20.
My November 22 report on this development can be read at:
Update on the status of the classification of PVFS, ME and CFS for ICD-11: Part Three: WHO rejects Dr Dua’s proposal
https://dxrevisionwatch.com/2018/11...d-11-part-three-who-rejects-dr-duas-proposal/
Last edited:
")
