ME Association: Forward ME and Oxford Brookes University Announce Results of Patient Survey on CBT and GET in ME/CFS | 03 April 2019
https://www.meassociation.org.uk/20...urvey-on-cbt-and-get-in-me-cfs-03-april-2019/
Lady Margaret Mar, Chair, Forward ME.
We are pleased to be able to let you see the results of the recent survey conducted on behalf of Forward-ME.
All the raw data was analysed and inserted into a comprehensive report by Professor Helen Dawes and Her team at Oxford Brookes University...
---------------
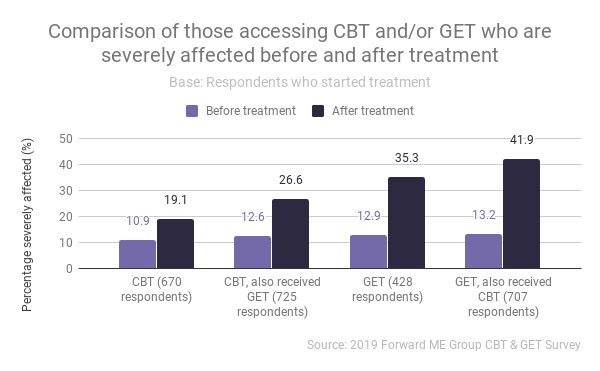
The conclusion includes –
“The results show clearly that cognitive behavioural therapy and graded exercise therapy are unsuitable treatments or management approaches for ME/CFS. The changes in severity and the worsening of symptoms are clear indications that the therapies being offered are having adverse effects on the health of individuals.”
https://www.meassociation.org.uk/20...urvey-on-cbt-and-get-in-me-cfs-03-april-2019/
Lady Margaret Mar, Chair, Forward ME.
We are pleased to be able to let you see the results of the recent survey conducted on behalf of Forward-ME.
All the raw data was analysed and inserted into a comprehensive report by Professor Helen Dawes and Her team at Oxford Brookes University...
---------------
The conclusion includes –
“The results show clearly that cognitive behavioural therapy and graded exercise therapy are unsuitable treatments or management approaches for ME/CFS. The changes in severity and the worsening of symptoms are clear indications that the therapies being offered are having adverse effects on the health of individuals.”